
Sorry, but I’m cheating on my diet and I don’t like loose ends
Sorry, but I’m cheating on my diet and I don’t like loose ends
I desire the things which will destroy me in the end – Sylvia Plath
http://www.economist.com/news/science-and-technology/21596923-how-babbling-babies-can-boost-their-brains-beginning-was-word
This observation has profound implications for policies about babies and their parents. It suggests that sending children to “pre-school” (nurseries or kindergartens) at the age of four—a favoured step among policymakers—comes too late to compensate for educational shortcomings at home. Happily, understanding of how children’s vocabularies develop is growing, as several presentations at this year’s meeting of the American Association for the Advancement of Science showed.
She measures how quickly toddlers process language by sitting them on their mothers’ laps and showing them two images; a dog and a ball, say. A recorded voice tells the toddler to look at the ball while a camera records his reaction. This lets Dr Fernald note the moment the child’s gaze begins shifting towards the correct image. At 18 months, toddlers from better-off backgrounds can identify the correct object in 750 milliseconds—200 milliseconds faster than those from poorer families. This, says Dr Fernald, is a huge difference.
Mind the gap
The problem seems to be cumulative. By the time children are two, there is a six-month disparity in the language-processing skills and vocabulary of the two groups. It is easy to see how this might happen. Toddlers learn new words from their context, so the faster a child understands the words he already knows, the easier it is for him to attend to those he does not.
It is also now clear from Dr Fernald’s work that words spoken directly to a child, rather than those simply heard in the home, are what builds vocabulary. Plonking children in front of the television does not have the same effect. Neither does letting them sit at the feet of academic parents while the grown-ups converse about Plato.
The effects can be seen directly in the brain. Kimberly Noble of Columbia University told the meeting how linguistic disparities are reflected in the structure of the parts of the brain involved in processing language. Although she cannot yet prove that hearing speech causes the brain to grow, it would fit with existing theories of how experience shapes the brain. Babies are born with about 100 billion neurons, and connections between these form at an exponentially rising rate in the first years of life. It is the pattern of these connections which determines how well the brain works, and what it learns. By the time a child is three there will be about 1,000 trillion connections in his brain, and that child’s experiences continuously determine which are strengthened and which pruned. This process, gradual and more-or-less irreversible, shapes the trajectory of the child’s life.
Fortunately, taciturnity can be easily fixed. Telling parents is the first step: many who volunteered themselves and their children for study did not know they could help their babies do well simply by speaking to them.
There are tools that can help, as well. One such is a Language Environment Analysis (LENA) device. It is like a pedometer, but keeps track of words, not steps, by analysing the speech children hear. It was originally developed as a prop for research, but parents kept asking for the data it recorded and researchers thus realised it could also serve as a spur. Parents use it to monitor, and improve, their patterns of speech, much as a pedometer-wearing couch potato might try to reach 10,000 steps a day, say.
A recent study by Dana Suskind shows how promising this approach is. Dr Suskind is a paediatric surgeon in Chicago. She got interested in the field while monitoring children whom she had fitted with artificial cochleas, to treat deafness.
Her new study shows that the use of a LENA device, combined with a one-off home visit to give parents advice, produces a 32% increase in the number of words a child hears per hour after six weeks. Dr Suskind’s Thirty Million Words Initiative (named after Dr Hart’s and Dr Risley’s original finding) is now using LENA devices and weekly home visits to improve the linguistic diet of children in Chicago. Parents are taught to make the words they serve up more enriching. For example, instead of telling a child, “Put your shoes on,” one might say instead, “It is time to go out. What do we have to do?”
Other groups are trying similar approaches. In Providence, Rhode Island, Angel Taveras, the mayor, has started a project that uses LENA devices to improve the vocabularies of children in pre-school. Meanwhile, in Chicago and several other places, nurses who visit mothers’ homes to give them advice on health and nutrition also encourage them to chat to their children and read to them aloud. Such interventions are effective and not particularly expensive.
In January Barack Obama urged Congress and state governments to make high-quality pre-schools available to every four-year-old. He is knocking on an open door. This financial year 30 states and the District of Columbia have increased spending on pre-schools. Nationally, this amounts to an increase of 6.9%.
That is a good thing. Pre-school programmes are known to develop children’s numeracy, social skills and (as the term “pre-school” suggests) readiness for school. But they do not deal with the gap in much earlier development that Dr Fernald, Dr Noble, Dr Suskind and others have identified. And it is this gap, more than a year’s pre-schooling at the age of four, which seems to determine a child’s chances for the rest of his life.
Not sure where this is from, but feel that tingle in the back of your head? That’s the feeling of your mind blowing up.
And so the slow, arduous public conversation task begins…
PDF: AFR_Healthcare20_BigDataRoundtable_140625
Story & Video: http://www.afr.com/p/business/healthcare2-0/leadership_vacuum_cripples_health_VrDsiSCDYOWXyuvg54QfJN
PUBLISHED: 19 JUN 2014 05:36:14 | UPDATED: 20 JUN 2014 05:18:23
MARK EGGLETON
Australia continues to struggle with the concept of e-health, with numerous health sector stakeholders equally to blame. This was one of the key messages to come out of the recent Big Data in Healthcare roundtable held by The Australian Financial Review in partnership with GE in Sydney.
Capital Markets CRC principal adviser Dr Paul Nicolarakis suggested part of the problem was Australia lacks a vision for healthcare. He suggested we don’t have someone or a collection of individuals working towards one goal. There are numerous stakeholders across the sector all vying to be the loudest voice, yet not pursuing a common goal.
Chief scientist at The George Institute for Global Health, Professor Anushka Patel said there was no one out there explaining and selling the potential value of big data and e-health or really engaging the government in a productive manner.
“There’s potential to reduce waste and reduce healthcare expenditure without sacrificing quality of care and health outcomes,” Professor Patel said.
“I also think big data could improve our ability to ensure equity, better health outcomes and health access. Those are the two of the big policy messages that need to be conveyed.”
Professor Enrico Coiera, who is the director of the Centre for Health Informatics, said data is already on the move – it just needs to be better linked. He said there is already plenty of data that’s slowly improving quality out there.
“The job is to get that moving around the system. Cheap fees and hospitals sharing information is what we want. Importantly, let’s drop the e from e-health and just improve health services,” Professor Coiera said.
Paul Nicolarakis reiterated that part of the problem was we lack strong, informed, insightful leaders of our health system.
“With all respect to the Australian Medical Association, they are not appointed to be the leaders of the health system. Our health ministers are not health people, they aren’t clinicians or experts in health, and I think, because of these sort of structural limitations, it’s very hard to develop the idea of e-health.
For the head of the Australian Healthcare and Hospitals Association, Alison Verhoeven, the time is ripe for change right now. She suggested that, with the federal Health Minister Peter Dutton talking about structural reform in the health system, the time is right to really address the big data question as it can help drive efficiency.
Verhoeven said a more streamlined system would see better consumer as well as clinician engagement.
“It’s about better system leadership as well.
“I’d really like to see a more integrated healthcare system generally come out of the structural reforms being discussed at the moment but whether that happens or not is another matter,” she said.
GE Healthcare Solutions managing director Dr David Dembo shares Verhoeven’s cautious view that we’re not going to see any real change in Australia.
“Unfortunately change happens very slowly in health and it happens slowly because free market principles don’t apply and because we don’t have strong leadership.
“We need to have people step up to the plate who are prepared to make brave and considered decisions, particularly around selling a vision and building a culture that gets buy-in from everybody – doctors, consumers and politicians.
“This journey we’re going on to take the ‘e’ out of e-health is the opportunity to de-fragment our health system and you only do that when everybody agrees this is a data science and this is our opportunity for health to behave as a system.”
The Australian Financial Review
Story: http://www.afr.com/p/business/healthcare2-0/privacy_fears_curb_health_growth_kxxq9sVuxrKDFz6enebgWP
PUBLISHED: 15 HOURS 46 MINUTES AGO | UPDATE: 14 HOURS 8 MINUTES AGO

“We have to be able to sell people a vision about why e-health is important to them,”, says Australian Healthcare and Hospitals Association CEO Alison Verhoeven. Photo: Reuters
MARK EGGLETON
In a twist on the old highwayman demand of “Your money or your life” we finally have an answer when it comes to e-health. Our personal finances win while our health takes a back seat.
Right now most Australians when they want to get a snapshot of their financial situation can go online and find up-to-the-minute information on their bank balance and outstanding debts. We’re pretty comfortable with the level of security afforded our financial details and even happy to give out further details if we’re keen on purchasing goods or services. Unfortunately, we’re a little leery about having our health records available online beyond what’s stored in a computer on our GPs desk.
Security of data was one of the major focuses of the recent Big Data in Healthcare roundtable held byThe Australian Financial Review in partnership with GE in Sydney with most participants agreeing it was an issue.
According to Australian Healthcare and Hospitals Association CEO, Alison Verhoeven, the best way to address people’s privacy concerns is better communication.
“We have to be able to sell people a vision about why e-health is important to them,” she says.
Furthermore, Verhoeven worries that while we continue to argue around the fringes of the debate we’re falling behind as technology moves on.
“The focus of discussion around e-health is on the desktop versions of e-health. We haven’t actually really begun to talk about the mobile versions of e-health so we’re really constructing a system that works on old technology,” Verhoeven says.
Part of the problem with Australia’s roll-out of some form of e-health framework was the personally controlled electronic health record (PCEHR) set up by the last federal government was it was poorly conceived and advertised, with very few Australians opting to participate.
Chief scientist at The George Institute for Global Health, Professor Anushka Patel says the best option would have been to give Australians the opportunity to opt out of the PCEHR rather than opt in.
In her experience in health services research it’s often very difficult to get opt-in consent, logistically, and opt-out consent is frequently used.
“Very few people opt out. Even in situations where opt-out can occur later in the course of the investigations very few people opt out. That’s a real test of whether people have real concerns such as privacy. I certainly think opt-out is the way to go,” Professor Patel said.
Director of the Centre for Health Informatics Professor Enrico Coiera says people do have a right to be a little apprehensive about data security and part of the problem is health services, especially government departments, don’t really “have their heads around the issue yet”.
For Paul Nicolarakis, the principal adviser from Capital Markets CMC and former senior adviser to Tanya Plibersek (the previous government’s health minister), the privacy question is an obvious concern. Yet he believes we have communicated the benefits of e-health in the wrong way.
“If e-health is valuable then it’s the same conversation as immunisation. It’s like everyone feels a bit of pain, you’ve got to go get your injections, but there’s value, which is you don’t get sick.
“If we can start framing an e-health record, as immunisation has been so brilliantly framed over the years, then I think people will get it. The analogy runs right through to there even being a kind of herd immunity granted to the population when everyone or most people are on board. The upside for the community is massive, and I don’t think that’s been articulated that well,” Nicolarakis says.
Interestingly, the US, which a few years ago was in last place in terms of implementing an e-health strategy, is now considered a leader in terms of policy sharpness and ensuring e-health has a positive impact.
The US has built the idea of “meaningful use” into the core of their electronic health record technology.
“It’s not talking about whether you have your boxes ticked in terms of what software you’ve got or what computers you have. It asks the question of whether the e-health record has a meaningful impact on patient care,” Nicolarakis says.
Dr Terry Hannan from the University of Tasmania and Launceston Hospital has seen the meaningful impact more connected health and better use of data can have on a number of projects around the world. He was the co-founder of the largest e-health system in the world for managing the AIDS epidemic of 40 million people in Africa.
“We’re now in over 200 countries in the world and we have a massive amount of standardised data for clinical day-to-day care, resource utilisation, research and outcomes. It’s now linked to the mobile health phenomenon and patients are using their own data via a mobile phone as a tool for improving their care.”
Hannan says similar programs have been rolled out in a number of communities in developing countries.
“In Pakistan, we track the multi-drug treatment for tuberculosis right down to the individual house and patient.
We can monitor the food that’s supplied to these impoverished people so they comply with their medication, all recorded on a mobile phone in a country with interrupted connectivity to the internet,” Hannan says.
The roundtable panel agreed the great potential of e-health lies in the preventative health sphere where the use of non-health data such as our nutrition habits could help revolutionise our future health outcomes.
Professor Patel says we could potentially link the quite extensive databases that already exist.
“We already have one for everything that’s available in any supermarket in Australia and a lot of that information was crowd-sourced – people with their mobiles.
“Link that to frequent user, loyalty programs that some of the big supermarkets have and we can look at what people spend at the check-out counter, and you can very accurately predict how levels of obesity are going to change due to the composition of people’s diet, their salt intake and more,” she says
“It allows you to target health outcomes at the policy level.”
Unfortunately, this hardly gets mentioned in the more emotive debates around privacy and the supposed infallibility of clinicians.
“Most of the unexplained variation in health research is from people who believe their own clinical insights and experience is of greater value than what might be data driven or might be evidence-based,” Patel says.
Verhoeven agrees and says moving our thinking away from anecdote-driven decision-making to data-driven decision-making is a real challenge for clinicians.
Professor Patel says the future starts now, but it requires a change of thinking across the profession.
“It is important this data driven approach to medicine is integral to the training of this current generation of doctors and healthcare professionals otherwise we’re not going to get the cultural change down the track.”
The Australian Financial Review
Vitality absolutely smash it across the board…
Must get on to these guys…..
PDF: Vitality_Recommendations2014_Report
PDF: InvestingInPrevention_Slides
Presentation: https://goto.webcasts.com/viewer/event.jsp?ei=1034543 (email: blackfriar@gmail.com)
From Forbes: http://www.forbes.com/sites/brucejapsen/2014/06/18/how-corporate-america-could-save-300-billion-by-measuring-health-like-financial-performance/
Bruce Japsen, Contributor
I write about health care and policies from the president’s hometown
The U.S. could save more than $300 billion annually if employers adopted strategies that promoted health, prevention of chronic disease and measured progress of “working-age” individuals like they did their financial performance, according to a new report.
The analysis, developed by some well-known public health advocates brought together and funded by The Vitality Institute, said employers could save $217 billion to $303 billion annually, or 5 to 7 percent of total U.S. annual health spending by 2023, by adopting strategies to help Americans head off “non-communicable” diseases like cancer, diabetes, cardiovascular and respiratory issues as well as mental health.
To improve, the report’s authors say companies should be reporting health metrics like BMI and other employee health statuses just like they regularly report earnings and how an increasing number of companies report sustainability. Corporations should be required to integrate health metrics into their annual reporting by 2025, the Vitality Institute said. A link to the entire report and its recommendations is here.
“Companies should consider the health of their employees as one of their greatest assets,” said Derek Yach, executive director of the Vitality Institute, a New York-based organization funded by South Africa’s largest health insurance company, Discovery Limited.
Those involved in the report say its recommendations come at a time the Affordable Care Act and employers emphasize wellness as a way to improve quality and reduce costs.
“Healthy workers are more productive, resulting in improved financial performance,” Yach said. “We’re calling on corporations to take accountability and start reporting health metrics in their financial and sustainability reports. We believe this will positively impact the health of both employees and the corporate bottom line.”
The Institute brought together a commission linked here that includes some executives from the health care industry and others who work in academia and business. Commissioners came from Microsoft (MSFT); the Robert Wood Johnson Foundation; drug and medical device giant Johnson & Johnson (JNJ); health insurer Humana (HUM); and the U.S. Department of Health and Humana Services.
The Vitality Institute said up to 80 percent of non-communicable diseases can be prevented through existing “evidence-based methods” and its report encourages the nation’s policymakers and legislative leaders to increase federal spending on prevention science at least 10 percent by 2017.
“Preventable chronic diseases such as lung cancer, diabetes and heart disease are forcing large numbers of people to exit the workforce prematurely due to their own poor health or to care for sick relatives,” said William Rosenzweig, chair of the Vitality Institute Commission and an executive at Physic Ventures, which invests in health and sustainability projects. “Yet private employers spend less than two percent of their total health budgets on prevention. This trend will stifle America’s economic growth for decades to come unless health is embraced as a core value in society.”
Duke story about direct monkey brain implants that allow the control of more than two arms.
Great take on dealing with lagging regulation:
“You shouldn’t ignore the laws. But if you worry as an investor about, “Oh, you shouldn’t invest in any personal genomics companies because there’s a lot of regulations that need to be updated.” Well, you won’t do anything innovative.”
So yes, absolutely, the regulations need to catch up with reality. I think as the outcomes of the science with Foundation Medicine, 23andMe, etc., start to become important to people and to patients, people will demand that change. And that’s how it happens.
http://recode.net/2014/06/21/google-ventures-bill-maris-on-moving-medicine-out-of-the-dark-ages/
Venture capital funding for the life sciences sector dropped by $5 billion from 2008 to 2012 and was basically flat last year, according to market reports. But the search giant’s venture arm, established in 2009, has steadily plugged money into companies throughout the space, including: 23andMe, Adimab, DNANexus, Doctor on Demand, Foundation Medicine,Flatiron Health, iPierian, One Medical Group, Predilytics, Rani Therapeutics, SynapDx and Transcriptic.
Some of the bets have started to pay off. Foundation Medicine raised $100 million in an initial public offering in 2013. Earlier this year, Bristol-Myers Squibb bought portfolio company iPierian in a deal that could be worth up to $725 million.
The focus on the space at least in part reflects the background of Google Ventures’Managing Partner Bill Maris. He studied neuroscience at Middlebury College and neurobiology at Duke University. In his early career, he was the health care portfolio manager at Swedish investment firm Investor AB.
Maris also took a lead role in the creation of Calico late last year, a Google-backed company focused on delaying aging and the diseases that come with it. (Google has declined to discuss the company, which is run by Genentech Chairman Arthur Levinson.)
“Medicine needs to come out of the dark ages now.”
Bill Maris, managing partner, Google Ventures
Google Ventures generally isn’t taking the old biotech route, betting on companies somewhere along the winding path of developing drugs that may — but probably won’t — someday earn Food and Drug Administration approval. Rather, the firm is focused on companies leveraging the increasingly powerful capacities of computer science, including big data, cloud processing and genomic sequencing, to improve diagnostics or treatments.
In the second part of my two-part interview, which has been edited for space and clarity, Maris discusses the promise of these tools for medicine as well as what’s still standing in the way.
Re/code: Looking through your health-care investments, there’s 23andMe, DNA Nexus, Foundation Medicine, Flatiron. To the degree there’s a common theme, it seems these are all big data plays, using a lot of information and smart algorithms to make advancements in medical research or hit upon more effective treatments. Is that part of your investment philosophy?
Maris: I used to be a health-care investor a long time ago in the public markets. One thing I learned that we tried to apply here is that investing in small molecules, trying to invest in the next treatment, there’s an element of gambling to that.
I’m glad that people started those companies and I’m glad that they have people who specialize in investing in them. But that’s not our specialty, because you have to build a portfolio to make a success overall.
What we try to put into our practice is “invest in what we know,” which is where health care meets technology. In some sense, almost all companies these days need to be big data companies.

Especially when you get around genomics or, like Flatiron, looking for insights across vast amounts of oncology data. These are by definition big data companies that couldn’t have existed 10 or 15 years ago.
Take Foundation Medicine. The tools didn’t exist to actually genotype quickly the way that we can today, and in 10 years it will be even more advanced. So by necessity the companies we’re investing in are in that space, because that’s the forefront.
Clinicians treating patients based on “if you present with these symptoms, I’m going to treat you based on the knowledge in my head?” Those days are either disappearing or will soon disappear, I hope. We can get much better outcomes from people if we understand the genetic basis of the exact cancer that they have, what interventions might be most effective against it, what’s worked in the past and what hasn’t. I think that’s where the future of health care is.
So yes, lots of these are big data companies, in that sense. But that’s a catchphrase, they’re more than that. They’re data-informed companies that are trying to build businesses that are commercially important and, in this case, relevant to patients. That means they’ll get better outcomes, you’ll live longer and be healthier.
Medicine needs to come out of the Dark Ages now.
There is a unique challenge when it comes to data and medicine. Either you have a lot of information that is stored away in paper filing cabinets in doctors’ offices, or you’ve got companies that did studies decades ago that might be of use but they’re either not digitized or they’re holding on to them as intellectual property. So while there’s this great potential, it’s actually really hard to get at it. Can you talk a bit about what needs to happen technologically?
Of course it’s difficult. If it were easy it would be done by now, there would be nothing remarkable about what Nat [Turner] and Zach [Weinberg] are doing at Flatiron. The fact that it’s difficult is what makes it something an entrepreneur needs to tackle — and this isn’t unique, right?
All the information in the world has been pretty dispersed, but Google’s mission has been to organize it and make it universally accessible. That’s kind of a crazy mission and they’re doing okay at it. It takes people with a vision to say, “We’re going to try to organize this and make it accessible to people.” When we do those things, good things will result from that.
Maybe it takes a generation, because doctors will start using the system. Or maybe it just takes one big push, where we’re just going to go into clinicians’ offices and help them get all the data organized and put into electronic formats. Once you’ve done it one time you can gain an infinite number of insights to help your patients, so there’s a good motivation to do that.
Organizing healthcare information is a daunting task, but it is not an impossible task. We’ve had people walk on the moon. This is a lot more doable.
I want to ask about 23andMe. We’ve seen a handful of companies in that space that have closed or haven’t gone anywhere, and 23andMe obviously hit a big wall with the FDA last year.
I don’t know what you’re talking about.
Yeah, I read it somewhere. But that was a big part of their business, can you talk about what their ongoing prospects are and what direction they could steer in?
Yeah, as I understand it, the heredity product is still available and we see big businesses being built there, like Ancestry.com and others.
At the same time, their vision is bigger than that. They’re at an impasse with the FDA right now, but no one has thrown up their hands. Communication is ongoing, they’re trying to work that out, we’re dedicated to trying to resolve that roadblock. And we think it’s a product that is of value to people, so they can look at and understand their own genomic information.
I think the company’s prospects are great, I’ve known [co-founder] Anne [Wojcicki] for almost 20 years now, and she’s nothing if not focused, dedicated and motivated. She’s a believer in this. I think the company has been a little bit ahead of its time.
![]()
It’s inevitable that everyone will eventually be genetically sequenced because it’s going to be really important to their health care, to understanding their future and what they’re at risk for. If you believe that, then you believe that there’s probably a big business to be built here because someone has to deliver that information.
So we have a lot of faith in the team.
Taking that case — and given that health care and medical research is moving in this digital direction — do you think there are some regulatory shifts that need to take place?
I think the laws need to catch up with science and reality, and the law is never good at that. It’s always slow.
I mean, look at the patent office. I just saw a patent that Smucker’s has for a peanut butter and jelly sandwich. It’s sort of crazy.
Look at Uber and its regulatory challenges, taxi and limousine commissions trying to stop Uber. When you sit with my job — which is a really fun job to do, kind of a judge at a science fair — it’s really important to look at the technology and how it might benefit people, and not worry about the bureaucracies that might try to impede that.
At the end of the day, what always happens is, the right products for society and the people get out there.
You shouldn’t ignore the laws. But if you worry as an investor about, “Oh, you shouldn’t invest in any personal genomics companies because there’s a lot of regulations that need to be updated.” Well, you won’t do anything innovative.
So yes, absolutely, the regulations need to catch up with reality. I think as the outcomes of the science with Foundation Medicine, 23andMe, etc., start to become important to people and to patients, people will demand that change. And that’s how it happens.
You studied neuroscience and neurobiology. What are some exciting developments you’re seeing in your own area?
I also think we’re just coming out of these Dark Ages in neuroscience. The forefront of neuroscience is (he points to parts of his head), “Well, this is the learning area, this is memory, this is where the right arm is controlled.” That’s not really how the brain works, it’s this cloud-based understanding.
I forget which neuroscientist said this, but you essentially have a Jennifer Aniston neuron. There are certain pathways in your brain that remember who that is. The more you fill up your brain with those things, the more neurons get used up.
So we’re getting closer to a point, and there are some folks at MIT working on this and other places as well, to really understanding the wiring of the brain. What makes it a whole, what causes consciousness. It’s not just that these cloudy regions all talk to each other.
You can’t do anything without a map. Until you can diagnose something you can never cure it, you can’t understand it. It’s hard to get from here to there without a map. So the first thing to do is to build a model.
When you can map an entire human brain, then you can really understand how it all works.

We don’t even know if everything gets recorded in your brain and your brain is just really good at controlling noise, where it’s just filtering out a bunch of things that you don’t need to think about because you’d just be overloaded. So there are these fundamental questions of neuroscience we just now have the tools to understand.
It’s so far behind, it’s so underfunded, in a way. We as a people and a country spend a lot of money on a lot of things. But we all walk around with this thing in our head and we have no understanding of how it actually works.
Machine-brain interfaces are a way to understand that. There’s a guy at Duke named Miguel Nicolelis, who I worked with and who comes out here every once in a while. He does work where he implants electrodes into brains and he’s now got monkeys who can move cursors on a screen [with virtual arms] and they get a reward of orange juice. Then he thought, “Well, why is the monkey just limited to one [virtual arm]? Maybe I could teach them to move three at once, or four.”
What we are learning from that is, well, we have two legs and two arms, but your brain is actually capable of operating four or six of them if you had them. There’s so much potential.
Here’s what the monkey saw in that experiment:
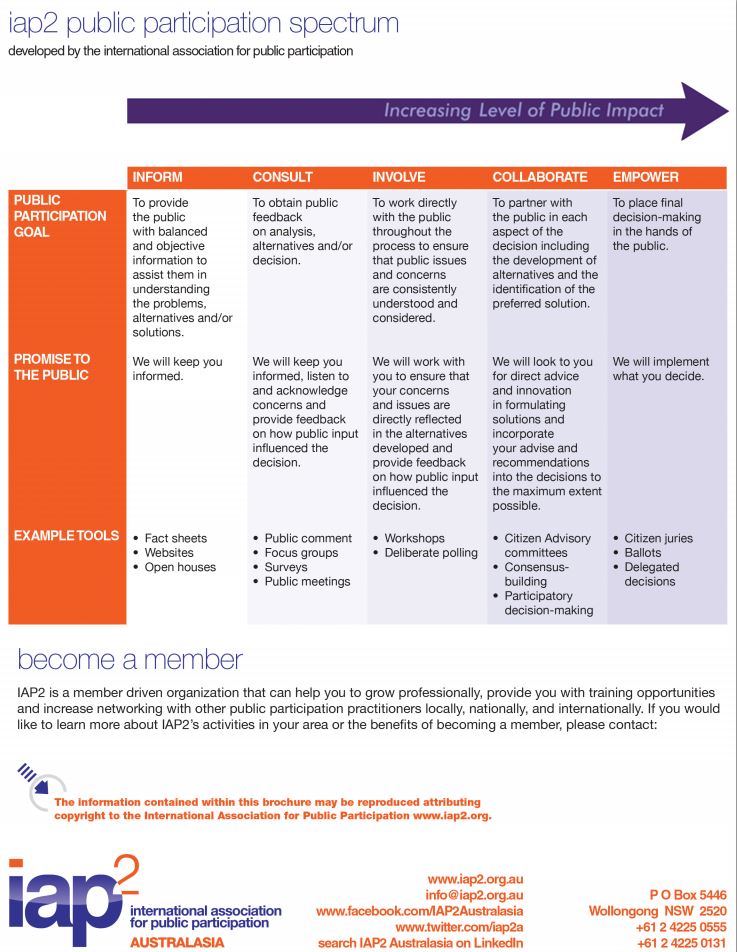
Interesting organisation and interesting framework for thinking about engagement with the public on particular issues… more than just specific technical engagement approaches… thanks Jen!
The International Association for Public Participation – Australasia: http://www.iap2.org.au/
Participation Spectrum: http://www.iap2.org.au/resources/iap2s-public-participation-spectrum
IAP2_PublicParticipationSpectrum
https://www.mja.com.au/insight/2014/22/high-lap-band-surgery-revision

http://t.co/g9LnZnM5ta
“Many people think that doctors make their recommendations from a basis of scientific certainty, that the facts are very clear and there’s only one way to diagnose or treat an illness,” he told the review. “In reality, that’s not always the case. Many things are a matter of conjecture, tradition, convenience, habit. In this gray area, where the facts are not clear and one has to make certain assumptions, it is unfortunately very easy to do things primarily because they are economically attractive.”

His wife, Dr. Marcia Angell, said the cause wasmelanoma.
Dr. Relman and Dr. Angell filled top editorial posts at the journal for almost a quarter-century, becoming “American medicine’s royal couple,” as the physician and journalist Abigail Zuger wrote in The New York Times in 2012.
The couple shared a George Polk Award, one of journalism’s highest prizes, for an article in 2002 in The New Republic that documented how drug companies invest far more in advertising and lobbying than in research and development.
His extended critique of the medical system was just one facet of a long and accomplished career. Dr. Relman was president of the American Federation for Clinical Research, the American Society of Clinical Investigation and the Association of American Physicians — the only person to hold all three positions. He taught and did research at Boston University, the University of Pennsylvania, Oxford and Harvard, where he was professor emeritus of medicine and social medicine.
Early in his career, he did pioneering research on kidney function.
He was also editor of The Journal of Clinical Investigation, a bible in its field, and he wrote hundreds of articles, for both professional journals and general-interest publications. Days before he died, Dr. Relman received the galleys of his final article, a review of a book on health care spending for The New York Review of Books, to which he was a frequent contributor.
In a provocative essay in the New England journal on Oct. 23, 1980, Dr. Relman, the editor in chief, issued the clarion call that would resound through his career, assailing the American health care system as caring more about making money than curing the sick. He called it a “new medical-industrial complex” — a deliberate analogy to President Dwight D. Eisenhower’s warning about a “military-industrial complex.”
His targets were not the old-line drug companies and medical-equipment suppliers, but rather a new generation of health care and medical services — profit-driven hospitals and nursing homes, diagnostic laboratories, home-care services, kidney dialysis centers and other businesses that made up a multibillion-dollar industry.
“The private health care industry is primarily interested in selling services that are profitable, but patients are interested only in services that they need,” he wrote. In an editorial, The Times said he had “raised a timely warning.”
In 2012, asked how his prediction had turned out, Dr. Relman said medical profiteering had become even worse than he could have imagined.
His prescription was a single taxpayer-supported insurance system, likeMedicare, to replace hundreds of private, high-overhead insurance companies, which he called “parasites.” To control costs, he advocated that doctors be paid a salary rather than a fee for each service performed.
Dr. Relman recognized that his recommendations for repairing the health care system might be politically impossible, but he insisted that it was imperative to keep trying. Though he said he was glad that the health care law signed by President Obama in 2010 enabled more people to get insurance, he saw the legislation as a partial reform at best.
The health care system, he said, was in need of a more aggressive solution to fundamental problems, which he had discussed, somewhat philosophically, in an interview with Technology Review in 1989.
“Many people think that doctors make their recommendations from a basis of scientific certainty, that the facts are very clear and there’s only one way to diagnose or treat an illness,” he told the review. “In reality, that’s not always the case. Many things are a matter of conjecture, tradition, convenience, habit. In this gray area, where the facts are not clear and one has to make certain assumptions, it is unfortunately very easy to do things primarily because they are economically attractive.”
Dr. Relman edited The New England Journal of Medicine from 1977 to 1991. Founded in 1812, it is the oldest continuously published medical journal in the world, reaching more than 600,000 readers a week. Dr. Angell was the editor in 1999 and 2000.
When he took the journal’s helm, interest in health news was booming, and newspapers and magazines competed to be first in reporting new developments. One policy he instituted was to ask general-interest publications not to disclose a forthcoming article in advance, a request almost always honored, albeit sometimes grudgingly.
He also began requiring authors to disclose any financial arrangements that could affect their judgment in writing about the medical field, including consultancies and stock ownership.
Dr. Relman and Dr. Angell met when she was a third-year student and he was a professor at Boston University School of Medicine. They published a paper on kidney disease together in The New England Journal of Medicine, then did not see each other for years.
After he became the journal’s editor, he asked her to come on board as an editor, which she did, abandoning her career as a pathologist. They began living together in 1994 — both were divorced by then — and married in 2009.
They became the ultimate medical power couple, not least because they were gatekeepers for one of the world’s most prestigious medical journals. Their outspoken views further distinguished them.
“Some have dismissed the pair as medical Don Quixotes, comically deluded figures tilting at benign features of the landscape,” Dr. Zuger wrote in The Times. “Others consider them first responders in what has become a battle for the soul of American medicine.”
Arnold Seymour Relman was born on June 17, 1923, in Queens (in an elevator, according to Dr. Angell) and grew up in the Far Rockaway neighborhood. His father was a businessman and avid reader who inspired his son’s love of philosophy. His mother nicknamed him Buddy, and friends called him Bud the rest of his life.
He skipped grades in school and graduated at 19 from Cornell with a degree in philosophy, but he chose not to pursue the field because it “seemed sort of too arcane,” his wife said. He earned a medical degree from the Columbia University College of Physicians and Surgeons at 22. His first marriage was to Harriet M. Vitkin.
In addition to Dr. Angell, he is survived by his sons, David and John, and a daughter, Margaret R. Batten, all from his first marriage; his stepdaughters, Dr. Lara Goitein and Elizabeth Goitein; six granddaughters; and four stepgrandsons.
Last June, Dr. Relman fell down a flight of stairs and cracked his skull, broke three vertebrae in his neck and broke more bones in his face. When he reached the emergency room, surgeons cut his neck to connect a breathing tube. His heart stopped three times.
“Technically, I died,” he told The Boston Globe.
He went on to write an article about his experience for The New York Review of Books, offering the unusual perspective of both a patient and a doctor.
“It’s both good and bad to be a doctor and to be old and sick,” he told The Globe.
“You learn to make the most of it,” he added. “Schopenhauer, the German philosopher, said life is slow death. Doctors learn to accept that as part of life. Although we consider death to be our enemy, it’s something we know very well, and that we deal with all the time, and we know that we are no different. My body is just another body.”


