All posts by blackfriar
Dubai offers gold for fat during Ramadan…
Good for them…
http://news.sky.com/story/1165863/gold-tips-scales-for-dubais-slimmers
Gold Tips Scales For Dubai’s Slimmers
More than £400,000 worth of gold was dished out to contestants in the Your Weight In Gold campaign, aimed at tackling obesity.

Ahmad al Sheikh took home 63g of gold after losing the most weight
Dubai dieters have been rewarded with gold for losing weight during the Muslim fasting month of Ramadan.
The Your Weight In Gold campaign gave away £474,000 worth of gold to about 3,000 contestants, who won one gram of gold for every kilogramme shed.
Contestants that lost more than five or 10 kg received a greater proportion of gold per kg.
Ahmad al-Sheikh, a 27-year-old Syrian architect, won the top prize of 63 grams of gold, worth £1,700, after he lost 26 kg.
“I actually registered 15 days later in the campaign and was worried at first, because I thought I lost a head start to all the other contestants,” he said.
He added that support from friends and family helped him achieve his goal.
“My friends and colleagues have also been of immense support when they found out I was trying to lose weight, so now I play football once a week and basketball twice every week as well,” he said.
Nearly 17 kg of gold was given away in the competition as more than 17,000 kg were shed by contestants.
Omar Ahmed al Marri, a public-relations executive from Dubai municipality, told The National that the gold was a key motivator in getting people to participate.
“Nobody tries to be healthy,” he said. “So we thought about how we could make them think about it. We found that you have to give them a gift, to motivate them.
“Most of the people, they first of all thought about the gold. And then afterwards, they thought about what they could do for their body.”
OECD: Health at a Glance 2013
- one of the highest life expectancies at birth of 82 years (2 years above the average)
- top five cancer survival rates
- top five AMI survival rates
- 8.9% health spend on GDP (OECD average: 9.3%)
- top three in rates of obesity – 28.3% (US – 36.5%; Mexico – 32.4%; NZ – 28.4%; UK – 24.8%)
- comparatively high rates of adverse events in hospitals – 8.6 per 100,000 (OECD average – 5)
- pressure on training pipeline, and eventually, health system financing
Medical Observer Summary:
- Use of cholesterol-lowering drugs: 1st, 50% above OECD avg
- Use of antihypertensives: 21st, 30% below OECD average
- Fatality within 30 days of acute MI: 5th lowest, 60% below OECD avg
- Use of antidepressants: 2nd, 59% above OECD avg
- Antibiotic prescribing in primary care: 8th, 17% above OECD avg
- Pharmaceutical expenditure per capita: 9th, 21% above OECD avg
- Remuneration of specialists: 3rd, 4.3 ratio to average wage
- Remuneration of GPs: 18th, 1.7 ratio to average wage
AU Media Release (PDF): Health-at-a-Glance-2013-Press-Release-Australia
OECD Report (PDF): Health-at-a-Glance-2013
Charts (PDF): Health-at-a-Glance-2013-Chart-set
OECD Source: http://www.oecd.org/health/health-systems/health-at-a-glance.htm
SMH (PDF): OECD says Australians take too many pills and must tackle nation’s obesity problem
Food Navigator: Psychology of satiety
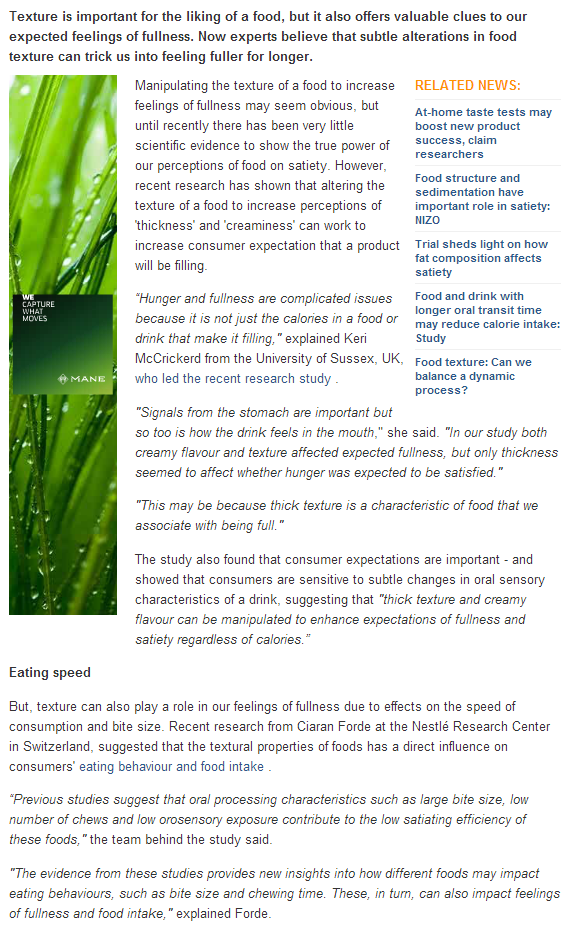
Texture and fullness: The psychology of satiety
Texture is important for the liking of a food, but it also offers valuable clues to our expected feelings of fullness. Now experts believe that subtle alterations in food texture can trick us into feeling fuller for longer.
http://www.foodnavigator.com/Science-Nutrition/Texture-and-fullness-The-psychology-of-satiety
FN: Longer oral transit time reduces calorie intake…
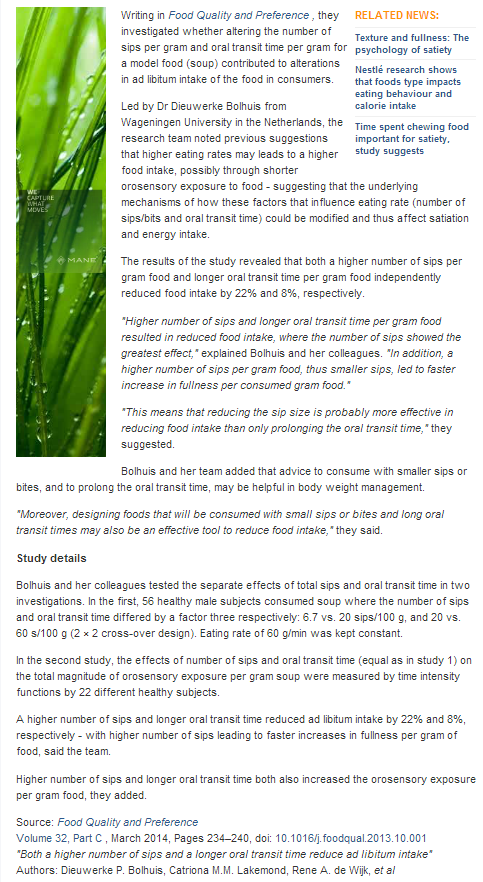
Food and drink with longer oral transit time may reduce calorie intake: Study
Designing foods and beverages to be consumed with small sips or bites, and a longer oral transit time, may be effective in reducing energy intake in consumers, say researchers.
Full article clip (copy/paste disabled by website):
Katz slam dunks….
- Used the Harvard Nurses Health Study to develop an algorithm for food healthiness as determined by health outcomes from the study – a GPS for nutrition – CLEVER!
- Offered to do this with Government in the early 2000s but was knocked back
- Developed a proprietary algorithm called ONQI, owned by NuVal
- Choosing higher scoring foods correlates with a lower risk of dying prematurely.
- “The very government agencies that regulate the food supply are extensively entangled with the entities producing our food, from farm to factory. In comparison, we mere eaters of food have very little clout. The government may be just a little too conflicted on the topic of food to be in the business of putting the truth, the whole truth and nothing but the truth on at-a-glance display.
Certainly the big food manufacturers, the makers of glow-in-the-dark snackattackables, should NOT be in the business of nutrition guidance whatever their inclination. That approach makes the fox look like a highly qualified security officer for the henhouse.
Which leaves independent nutrition, and public health experts and private sector innovation. And here we are.
Private-sector innovation often involves intellectual property, trade secrets and patent applications. It involves some entity making an investment and wanting a return. That is all true of NuVal, for better or worse. It wasn’t my plan – it was just the only way to get this empowering system into the hands of shoppers. Of note, the ONQI remains under the independent control of scientists, and not the business.” - This is a terrific strategy – worthy of emulation.
Nutrition Guidance: Who Needs to Know What?
DAVID L. KATZ June 11, 2013
I am writing today about nutrition guidance and who needs to know what to make it useful.
Permit me to disclose right away that I am the principal inventor of the Overall Nutritional Quality Index (ONQI) algorithm, used in NuVal – a nutritional guidance system that stratifies foods from 1 to 100 on the basis of overall nutritional quality: the higher the number, the more nutritious the food. As the Chief Science Officer for NuVal, LLC, I am compensated for my continuous and considerable allocations of time and effort. But it was never supposed to be that way – and the reasons why it is are an important part of this story.
As to why this column now, there are two recent provocations. One is our ongoing work to complete the updated algorithm, ONQI 2.0, and the window that provides into a world of weirder foods than I ever even considered possible. The other is a paper published in the Journal of the Academy of Nutrition and Dietetics a few months back and a more recent exchange of letters related to that article. The article described the advantageous novelties of a nutritional profiling system, such as weighting nutrients for their health effects rather than counting them all the same. But this was less about novelty, and more about NuVal, since the innovations described have long been included in the ONQI.
[See: Debunking Common Nutrition Myths.]
Claims about alleged novelties that were already included in NuVal prompted a letter from my colleagues and me to the journal, which was published along with a response from the original authors. In that response, they acknowledged that the NuVal system included the so-called “novelties” and acknowledged that the ONQI is, to date, the only nutritional profiling system shown to correlate directly with health outcomes. So the real concern, the letter went on, is that the ONQI algorithm is proprietary and the details are not fully in the public domain.
Which brings us back to why NuVal is a private and proprietary system in the first place and whether or not it matters that certain details of the algorithm – which populate 25 pages or so of computer code written in a language called SAS – are not on a billboard. Why isn’t the ONQI public rather than private, and who really needs to know every detail of the algorithm for it to be useful? (All of the nutrients included in it, and the basic approaches used to generate scores, have been published.)
The ONQI, and NuVal, are a private sector innovation because the public sector said: no thanks. In 2003, I was privileged to be a member of a group of 15 academics invited to Washington, D.C. by then-Secretary of Health Tommy Thompson. A Food and Drug Administration task force had been formed to guide efforts related to the control of rampant obesity and diabetes, and we were a part of that effort. We gathered in a conference room with Secretary Thompson, the FDA Commissioner (Mark McClellan) and others, including the surgeon general and the heads of the National Institutes of Health and the Centers for Disease Control and Prevention.
[See: Why Aren’t Americans Healthier?]
We were each given one three-minute turn to offer up one good idea the FDA and other federal agencies might use to help combat the ominoustrends in diabetes and obesity. I used my turn to describe, in essence, the project that later became the ONQI. I suggested that the secretary might convene a totally independent group of top-notch experts in nutrition and public health, perhaps under the auspices of the Institute of Medicine.
The group should have no political or industry entanglements and should be allowed to work for as long as it took to convert the best available nutrition science and knowledge into a guidance system anyone could understand at a glance. I was thinking, in essence, of the equivalent of GPS for nutrition, so that no one trying to identify a better food in any given category would get lost, confused or misled by Madison Avenue.
[See: 10 Things the Food Industry Doesn’t Want You to Know.]
I waited two years for the feds to do something along these lines. When they didn’t, I decided to undertake the project myself, with the backing of Griffin Hospital in Derby, Conn. – a Yale-affiliated, not-for-profit community hospital, which owns the ONQI algorithm to this day. Other than this being a private rather than federal endeavor, all other aspects of the project were just as proposed to the U.S. Secretary of Health. When we completed the algorithm, I offered it again to the FDA. A scientist at the agency recommended a private-sector approach if I hoped to live long enough to see the system do its intended good.
Why didn’t the feds take on the project? We can all conjecture. I suspect it has something to do with the story Marion Nestle told us all in Food Politics, and the stories we routinely hear about the Farm Bill from the likes of Michael Pollan, Mark Bittman and others. The very government agencies that regulate the food supply are extensively entangled with the entities producing our food, from farm to factory. In comparison, we mere eaters of food have very little clout. The government may be just a little too conflicted on the topic of food to be in the business of putting the truth, the whole truth and nothing but the truth on at-a-glance display.
[See: Seeking a More Perfect Food Supply.]
Certainly the big food manufacturers, the makers of glow-in-the-dark snackattackables, should NOT be in the business of nutrition guidance whatever their inclination. That approach makes the fox look like a highly qualified security officer for the henhouse.
Which leaves independent nutrition, and public health experts and private sector innovation. And here we are.
Private-sector innovation often involves intellectual property, trade secrets and patent applications. It involves some entity making an investment and wanting a return. That is all true of NuVal, for better or worse. It wasn’t my plan – it was just the only way to get this empowering system into the hands of shoppers. Of note, the ONQI remains under the independent control of scientists, and not the business.
[See: Mastering the Art of Food Shopping.]
Which leads us back to the second question: Is it a problem for a system like this to be a private-sector innovation? Who, really, needs to know every detail of such an algorithm?
Consider that if you are shopping for a car, you do need to know if it comes with anti-lock brakes or all-wheel drive. But to decide if these are working for you, you don’t need engineering blueprints; you just need to drive in the snow. When shopping for a smartphone, you may want to know if it has GPS. But you don’t need the trigonometry equations on which the GPS is based to determine if it works; you just have to see if it helps you get where you want to go.
Nutrition guidance in general, and NuVal in particular, are just the same. What are the exact formula details? Who cares. We routinely rely on tools based on math and engineering most of us don’t understand – but we don’t need all that input to know if the tools are working for us. We just need the output. We need to be able to use them. People using NuVal have lost more than 100 pounds, and even over 200 pounds. Choosing higher scoring foods correlates with a lower risk of dying prematurely. More than 100,000 scores are on public display in 1,700 supermarkets nationwide. The ONQI is at least as transparent as any car or smartphone or computer.
[See: The No. 1 Skill for Weight Management.]
Let’s acknowledge: If you are reading this on a computer screen, neither of us truly understands the engineering involved in me writing it, using word processing software, attaching it to an email and sending it to my editor at U.S. News & World Report so she could post it in cyberspace, where you found it. But we do know it worked.
We rely on private-sector innovation for a lot of important jobs, and even many that put our safety on the line. The private sector makes our cars and planes. We seem to be comfortable using these without scrutinizing patent applications. The private sector makes our computers, and smartphones and GPS systems, and we can tell whether or not these work, even if we don’t know how.
Why, then, is nutrition guidance different? The answer, I believe, is politics, profits and the inertia of the status quo. We are accustomed to vague nutrition guidance from conflicted sources, and those same sources are apt to imply there is something wrong with private-sector innovation and the intellectual property issues that come along with it. But if those issues don’t undermine the cars, and planes and navigation systems that get us from city to city and coast to coast, it’s not at all clear why they should be a problem when navigating among choices in a supermarket aisle.
[See: The Government’s MyPlate Celebrates Second Birthday.]
As a scientist, and not a businessperson, my preference would be to put the ONQI on a billboard for all the good it would do. But on this, I must defer to the businesspeople who have made the relevant investments and are entitled to safeguard potential returns. As for the scrutiny that all advanced systems should get, the ONQI has been shared with scientists at leading universities and health agencies around the world – but for private assessment and use rather than public display. Others like them who want to review the program need only ask.
We should all care that the military-industrial establishment seems opposed to putting the blunt truth about nutritional quality, as best we know it, on at-a-glance display. We should care that federal authorities responsible for nutrition guidance are also responsible, if only indirectly, for food politics and supply-side profits. That story may lack novelty. It may be old news. But it is nonetheless something everyone who eats does need to know – engineering blueprints not required.
Medical Body Area Network
- The FCC has proposed the allocation of spectrum for Medical Body Area Network (MBAN) devices.
- Deloitte expects the wireless health device market to triple in the next few years
3. Wireless body monitoring
We need only to listen to the words of FCC chairman Julius Genachowski to get a feel for the potential for wireless body monitoring. Genachowski noted last year that “a monitored hospital patient has a 48% chance of surviving a cardiac arrest,” compared with only 6% for an unmonitored patient.
With the tremendous opportunity for improving health care in mind, the FCC proposed allocating spectrum for Medical Body Area Network, or MBAN, devices. Such devices will record vital signs and other important physical information through sensors attached to a person’s body, with the data transmitted to a local wireless hub. The information can then be monitored remotely by clinical professionals, with alerts sent to let these experts know when medical intervention could be needed.
GE Healthcare (NYSE: GE ) is one company already developing MBAN devices. The giant company plans to introduce technology using sensors that monitor heart and breathing rates, temperature, and pulse oximetry within the next few years. Deloitte predicts that the wireless body monitoring market could more than triple in just the next couple of years. Within the next decade, this technology could be key in helping control overall medical costs.
China’s plans universal health care by 2020
China is expanding its health care system and aiming for universal coverage for its 1.35 billion citizens by 2020. The report estimates that the country alone will make up 34% of the global growth in medication spending over the next five years.
Source: http://healthland.time.com/2013/11/19/why-were-spending-1-trillion-on-health-medications/
Report PDF: IIHI_Global_Use_of_Meds_Report_2013
The 10 corporations that make everything…

This likely reflects the state of play pre-2012 (does not show Pringles sale to Kelloggs).

This does not reflect the Disney purchase of Lucasarts.

Full image: http://blog.panicola.com/wp-content/uploads/2013/11/Big-Food.jpg
Because in health, less is more…
When we look back at contemporary health systems 50 years from now, we will consider them to be an technologically indulgent folly of grand proportions, driven by an imperative to deliver more and more complex care in order to justify higher and higher costs.
In a fee-for-service context, elaborate technologies justify higher costs. An elective angiogram costs $25,000. If this had to be paid by individuals, there would be no interest in conducting them with the frequency that they are performed today.
Perhaps this is why Singapore, with its health savings accounts with health costing around 4% of GDP (achieving the same high outcomes of Australia), lacks the excesses of more universal health systems?
The use of bariatric surgery for obesity is perhaps the most egregious example of this phenomenon. A AU$20,000 – 30,000 procedure is now introducing moral hazard that will undermine attempts to introduce behavioural and lifestyle change i.e. “Why bother changing my lifestyle when I can simply get a lap band to fix me later?”
Pharmaceutical companies are also using this play book with the introduction of their new, highly-specialised, so-called “biologics” to the market, particularly in the cancer area. They are often protein based and extremely difficult to manufacture, but are also very targeted. Funders are responding to this threat with value-based payment schemes where by the drug company only gets paid if the treatment succeeds.
Current health market settings establish this perverse incentive. Moves to value/outcomes-based care will remedy these perversities, providing incentives for activities that reduce care costs. In such an environment, the cheapest interventions also become the most profitable.
Home delivered broccoli instead of lap-bands.
CBT SMS’s instead of SSRIs and psychotherapy.
A rapid learning health system instead of a profit yearning sickness market.