The women were asked to rate the amount of light in their bedrooms at night as:
Light enough to read
Light enough to see across the room, but not read
Light enough to see your hand in front of you, but not across the room
Too dark to see your hand or you wear a mask
Their answers were compared to several measures of obesity. Body Mass Index, waist-to-hip ratio and waist circumference were all higher in women with lighter rooms.
Prof Anthony Swerdlow, from the Institute of Cancer Research, told the BBC: “In this very large group of people there is an association between reported light exposure at night and overweight and obesity.
“But there is not sufficient evidence to know if making your room darker would make any difference to your weight.
“There might be other explanations for the association, but the findings are intriguing enough to warrant further scientific investigation.”
Body Clock
One possible explanation is that the light is disrupting the body clock, which stems from our evolutionary past when we were active when it was light in the day and resting when it was dark at night.
Light alters mood, physical strength and even the way we process food in a 24-hour cycle.
Artificial light is known to disrupt the body clock by delaying the production of the sleep hormone melatonin.
Prof Derk-Jan Dijk, from the Surrey Sleep Centre, said there would be no harm in trying to make bedrooms darker.
He told the BBC: “People in general are not aware of the light present in their bedroom, I think people should assess their bedroom and see how easy it would be to make it darker.”
Street lights, some alarm clocks and standby lights on electrical equipment such as televisions could light a room, he said.
“Overall this study points to the importance of darkness,” he concluded.
Cancer
The study was funded by Breakthrough Breast Cancer and the findings emerged from a long-term study to understand the risk factors for breast cancer. Obesity is known to increase the odds of the disease.
Dr Matthew Lam, from the charity, commented: “It’s too early to suggest that sleeping in the dark will help prevent obesity, a known risk factor for breast cancer, but the association is certainly interesting.
“Whilst we are learning more and more each day about the environmental, genetic and lifestyle factors that affect breast cancer risk, it is not yet possible to predict who will get breast cancer, and for women who have been diagnosed with the disease, we can’t yet say what caused it.”
Why are so many people overweight? Part of the reason, some think, is because they don’t have access to, the money to buy, or the desire to eat fresh fruits and vegetables.
That’s the idea behind initiatives like the “One more a day pledge” (whose slogan sounds like the pledge-taker might already be choking on carrots: “I pledge to eat … and help my family eat … at least ONE MORE fruit or veggie every day.”[ellipses sic])
Produce is less calorically dense than grains, meat, and fat, so increasing its consumption might indeed make sense as an obesity-fighting strategy—that is, if eating more fruits and vegetables caused people to compensate by eating fewer cookies and french fries.
Unfortunately, though, we don’t really eat that way. We’ll have a tossed salad—and thena Chipotle Quesarito. At least, that’s what RAND health economist Roland Sturm found in a new paper he co-authored with Ruopeng An, a health policy professor at the University of Illinois at Urbana-Champaign.
“Conventional wisdom is an awful guide for policy,” Sturm told me. “The consumption of fruits and vegetables has increased during the obesity epidemic.”
Differences in diet, such as eating more Cheetos and fewer cucumbers, help explain why some individuals are more obese than others, Sturm said. But they don’t explain why obesity has grown across all populations in nearly all U.S. states over the past few decades.
The study, published in the journal CA: A Cancer Journal for Clinicians, found that while college-educated people are still less likely to be obese than their less-educated counterparts, they’re still fatter than they used to be:
Increase in body mass index over time for people of various levels of education (CA: A Cancer Journal)
And the BMIs of the uber-healthy Coloradans, who regularly appear on “healthiest states” lists, have been rising over time, just like those of Mississippians have:
Prevalence of overweight over time in California, Colorado, and Mississippi. (CA: A Cancer Journal)
Today, people eat about 30 more pounds of vegetables and 25 more pounds of fruit per year than they did in 1970, according to Sturm’s calculations.
Unfortunately, they’re eating more of everything else, too. The average adult consumed about 2,100 calories in 1970, but in recent years that number has risen to more than 2,500.
Average daily per capita calories, adjusted for waste (CA: A Cancer Journal for Clinicians)
Attempts to discourage the consumption of certain macronutrients also don’t seem to work. Historically, people have simply eaten less of the forbidden substance and more of the others. During the low-fat craze of the 90s, for example, fat consumption dipped, but carbohydrate intake skyrocketed. And after the Atkins diet took off in 2000, people simply swapped carbs back in for fat.
Change in macronutrient consumption over time. (CA: A Cancer Journal for Clinicians)
“Preventing obesity is not about eating more food, regardless of how many nutrients it provides,” Sturm and An write, “but consuming less energy or expending more.”
Past research on the produce-obesity issue has been mixed: A 2003 study of a large sample of children found that eating more fruits and vegetables had no significant impact on weight. Around the same time, a different study of middle-aged nurses found those who ate more produce were less likely to become obese.
Sturm emphasized that his study is different because it’s looking at top-level changes over time, not disparities between groups of people.
A recent Lancet study found that rich and poor countries alike are now struggling with obesity, and that there have been “no national success stories” in stemming the epidemic. So while it’s definitely a problem that, say, poor American women tend to be fatter than richer women, another frightening trend is the overall rise of large waistlines over time.
Proteus occupy an interesting position… ingestibles are the ultimate in wearables. It’s smart also to be backed a big flailing incumbent player. It will be interesting to see if this stuff works.
Andrew Thompson on transforming healthcare at Wired Health 2014
Published On: May 5, 2014
Watch Proteus CEO Andrew Thompson present at Wired Health 2014 on transforming healthcare through digital medicines: http://bit.ly/1lS7RLe
WIRED Health is a one-day summit designed to introduce, explain and predict the coming trends facing the medical and personal healthcare industries. The inaugural event was held on Tuesday April 29, at the new home of the Royal College of General Practitioners, 30 Euston Square, London.
Withdrawing from measures we know will work in order to fund new measures we think might work seems a daft way to manage our health. But it’ll help cut the deficit.
It took Mark Latham to say the unsayable. “If a cure to cancer is to be found, most likely it will happen in Europe or the United States,” he wrote in the Weekend Financial Review. Spending scarce funds to find a cure ourselves is a waste of money, a political fig leaf to cover the electoral pain of the GP co-payment.
Anyone who doubts that the Medical Research Future Fund is a fig leaf or an afterthought, needs to only look at the pattern of leaks and speeches leading up to the budget. Ministers spoke often about the need to restrain the cost of Medicare, scarcely at all about the need to boost medical research.
They weren’t able to prepare the way for the medical research future fund because it didn’t come first. It isn’t that pharmaceutical benefits, doctors rebates and future hospital funding are being cut to pay for the fund. It’s that the fund was evoked late in the piece to smooth the edges of the cuts.
Under the descriptions of 23 separate cuts in the budget are the words: “The savings from this measure will be invested by the government in the Medical Research Future Fund”.
The cuts hit dental health, mental health, funding for eye examinations, measures to improve diagnostic images, research into preventive health, a trial of e-health and $55 billion of hospital funding over the next 10 years.
The wonders of budget accounting mean that the savings notionally allocated to the fund will actually be used to bring down the budget deficit except for when money is withdrawn from the fund to pay for research.
It’s the same trick Peter Costello pulled with the Future Fund. The government gets two gold stars for the price of one. It can both cut the deficit and build up the funds for medical research. And it isn’t yet too sure about what type of research.
Under questioning by senators on Monday, health department officials revealed that they didn’t even know about the fund until late in the budget process and even then provided no advice on how it would work.
Asked about the kind of things the fund would finance, the department’s secretary Jane Halton said the questions were hypothetical.
Would it include evaluations of potentially life-saving preventive health measures such as SunSmart and anti-tobacco programs? “I think it’s unlikely based on the description I have seen, but again we are in an area that we probably can’t yet answer,” she replied.
A few minutes later she asked for her words to be expunged saying she really didn’t know. “We need to work through this level of detail” she told the senators.
We know that cures for cancer, Alzheimer’s and heart disease will be part of fund’s remit, because the Treasurer told us so. “One day someone will find a cure for cancer,” he said after the budget. “Let it be an Australian and let it be us investing in our own health care.”
Latham’s point is that the idea is silly. By all means contribute proportionately to a global effort to find cures for diseases, but don’t try and lead the pack by taking scarce dollars away from applying the medical lessons we have already learnt.
Small countries like Australia are for the most part users rather than creators of technology, and our funds are limited as Joe Hockey well knows.
The Medical Journal of Australia isn’t fooled. This month’s editorial says a government genuinely concerned about extending the working lives of Australians would be investing more in preventing chronic disease, not less.
“The direct effects of the proposed federal budget on prevention include cuts to funding for the National Partnership Agreement on Preventive Health, loss of much of the money previously administered through the now-defunct Australian National Preventive Health Agency, and reductions in social media campaigns, for example, on smoking cessation,” it says.
“Increased funding for bowel cancer screening, the Sporting Schools initiative, the proposed National Diabetes Strategy and for dementia research are positive developments, but do not balance the losses.”
It’s the indirect effects of the measures the fund seeks to make palatable that have it really worried. The $7 co-payment will work out at $14 for patients with chronic diseases. They’ll pay once to see the doctor and then again to have a test. The editorial quoted four studies which have each found that visits for preventive reasons are the ones co-payments are most likely to cut back.
“The effects of these co-payments on preventive behaviour are greatest among those who can least afford the additional costs,” it observes. Which is a pity because “the potential for prevention is greatest among poorer patients, who are often at a health disadvantage”.
We’ll all suffer if co-payments cut vaccination rates, even those of us who aren’t poor, and even if the Medical Research Future Fund finds a cure cancer.
The journal’s biggest concern is that the cuts to hospital services will hit preventive health measures because they are seen as less urgent.
“The greatest pity of all is that the proposed cuts to funding for health come at the time when the first evidence is at hand of potential benefits of the large-scale preventive programs implemented under the national partnership agreements,” the journal writes. “A slowing in the rate of increase in childhood obesity and reductions in smoking rates among indigenous populations have been hard-won achievements.”
Withdrawing from measures we know will work in order to fund new measures we think might work seems a daft way to manage our health. But it’ll help cut the deficit.
The Big Fat Surprise: Why Butter, Meat and Cheese Belong in a Healthy Diet. By Nina Teicholz. Simon & Schuster; 479 pages; $27.99. Buy from Amazon.com,Amazon.co.uk
“EATING foods that contain saturated fats raises the level of cholesterol in your blood,” according to the American Heart Association (AHA). “High levels of blood cholesterol increase your risk of heart disease and stroke.” So goes the warning from the AHA, the supposed authority on the subject. Governments and doctors wag their fingers to this tune the world over. Gobble too much bacon and butter and you may well die young. But what if that were wrong?
Nina Teicholz, an American journalist, makes just that argument in her compelling new book, “The Big Fat Surprise”. The debate is not confined to nutritionists. Warnings about fat have changed how food companies do business, what people eat, and how and how long they live. Heart disease is the top cause of death not just in America, but around the world. The question is whether saturated fat is truly to blame. Ms Teicholz’s book is a gripping read for anyone who has ever tried to eat healthily.
The case against fat would seem simple. Fat contains more calories, per gram, than do carbohydrates. Eating saturated fat raises cholesterol levels, which in turn is thought to bring on cardiovascular problems. Ms Teicholz dissects this argument slowly. Her book, which includes well over 100 pages of notes and citations, covers decades of nutrition research, including careful explorations of academics’ methodology. This is not an obvious page-turner. But it is.
Ms Teicholz describes the early academics who demonised fat and those who have kept up the crusade. Top among them was Ancel Keys, a professor at the University of Minnesota, whose work landed him on the cover of Time magazine in 1961. He provided an answer to why middle-aged men were dropping dead from heart attacks, as well as a solution: eat less fat. Work by Keys and others propelled the American government’s first set of dietary guidelines, in 1980. Cut back on red meat, whole milk and other sources of saturated fat. The few sceptics of this theory were, for decades, marginalised.
But the vilification of fat, argues Ms Teicholz, does not stand up to closer examination. She pokes holes in famous pieces of research—the Framingham heart study, the Seven Countries study, the Los Angeles Veterans Trial, to name a few—describing methodological problems or overlooked results, until the foundations of this nutritional advice look increasingly shaky.
The opinions of academics and governments, as presented, led to real change. Food companies were happy to replace animal fats with less expensive vegetable oils. They have now begun abolishing trans fats from their food products and replacing them with polyunsaturated vegetable oils that, when heated, may be as harmful. Advice for keeping to a low-fat diet also played directly into food companies’ sweet spot of biscuits, cereals and confectionery; when people eat less fat, they are hungry for something else. Indeed, as recently as 1995 the AHA itself recommended snacks of “low-fat cookies, low-fat crackers…hard candy, gum drops, sugar, syrup, honey” and other carbohydrate-laden foods. Americans consumed nearly 25% more carbohydrates in 2000 than they had in 1971.
In the past decade a growing number of studies have questioned the anti-fat orthodoxy. Ms Teicholz’s book follows the work of Gary Taubes, a science journalist who has cast doubts on the link between saturated fat and health for well over a decade—and been much disparaged for his pains. There is increasing evidence that a bigger culprit is most likely insulin, a hormone; insulin levels rise when one eats carbohydrates. Yet even now, with more attention devoted to the dangers posed by sugar, saturated fat remains maligned. “It seems now that what sustains it,” argues Ms Teicholz, “is not so much science as generations of bias and habit.”
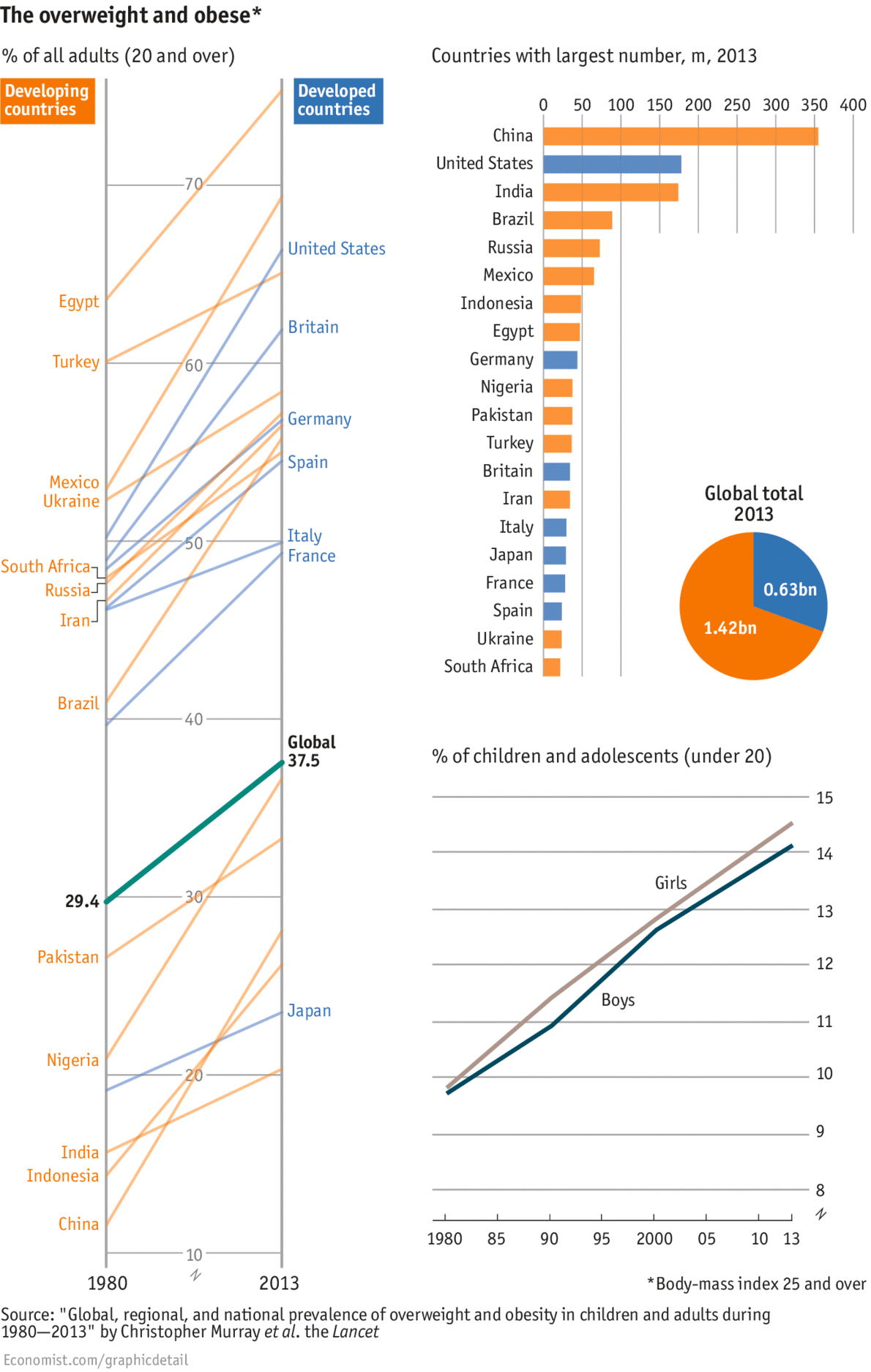
Worryingly, the study—led by the Institute of Health Metrics and Evaluation at the University of Washington—showed that children are fattening at a faster pace than adults. Last week the World Health Organisation set up a new commission to curb child obesity. But it will be some time yet before the world reaches peak fat.
WAISTLINES are widening everywhere. The percentage of adults who are overweight or obese has swelled from 29% in 1980 to 37% in 2013, according to a new study in the Lancet. People in virtually all nations got larger, with the biggest expansions seen in Africa, the Middle East and New Zealand and Australia. The chunkiest nations overall are found in the tiny Pacific islands and Kuwait, where over three-quarters of adults are overweight and over half are obese. And the world is unlikely to slim down soon. While the rate of increase has slowed in the rich world, it is still rising in poorer countries, where two-thirds of the world’s 2.1 billion overweight adults live. China is home to the largest number anywhere—335m, more than the population of America. This is not just because of its sheer size, but also because economic growth led to cellulite growth: a quarter of adults are now overweight compared with one in ten in 1980.Mexicans just outweigh neighbouring Americans. In both countries, two-thirds of people could lose a pound or two, though more Americans are obese. Agreeing on how to combat the problem is tricky, given that experts continue to bicker on what, precisely, makes us fat. Worryingly, the study—led by the Institute of Health Metrics and Evaluation at the University of Washington—showed that children are fattening at a faster pace than adults. Last week the World Health Organisation set up a new commission to curb child obesity. But it will be some time yet before the world reaches peak fat.
Frozen food includes a caloric deficit when eaten – the energy to melt it down. In a 100 cal dessert, this can account for up to a quarter of the calories. Go figure
Eating ice actually burns calories because it requires energy for the body to melt the cube. One curious doctor suggests this can be used as a legitimate weight-loss tool.
When he became determined to lose weight, Dr. Brian Weiner decided to change his eating and exercise regimes. “One of the first changes I made,” explains Weiner, a gastroenterologist in New Jersey and assistant professor at Robert Wood Johnson Medical School, “was to give up my beloved ice cream.”
Aiming for something lighter, Weiner replaced it with Italian ices. The cups at his supermarket listed their calorie content as 100—calculated by multiplying 25 grams of carbohydrate by four calories per gram. “One evening, in a burst of insight,” Weiner writes, “I realized that this calculation was incorrect. The manufacturer of the ices did not calculate the energy required to melt the ice, and did not deduct this from the calorie calculation.” By Weiner’s math, he was actually only consuming 72 calories, or “icals,” his term for the net caloric content of ice-containing foods after considering the calories that the body burns to produce the thermal energy that melts the ice.
Weiner reviewed the medical literature. “I found that no one has clearly identified this oversight,” he writes. “I could not locate references to considerations of the implications of the energy content of ice as food.”
After discussing the issue in detail with his son, an engineering student at Rutgers who vetted his father’s calculations, Weiner submitted his story as a letter to editors of the widely-read medical journal Annals of Internal Medicine. They published it. In the article, Weiner said the idea could be of real importance to people trying to lose weight. It’s meant as a supplement to overall diet and lifestyle that go into maintaing a healthy physical form. “While eating ice, you are serving two purposes,” Weiner explains, “you are burning calories and not eating positive-calorie foods.”
Now Weiner has also written an e-book, The Ice Diet. It’s free—part of his stated wish “not to get lumped in with the counter-productive fad diet (snake oil) promoters.”
As a practicing gastroenterologist, Weiner says he regularly avoids micromanaging food selection. He manages obesity as an illness and diets as part of a holistic approach to good eating. “I would usually cringe when patients brought up the weight loss diet of the day, usually some poorly documented and improbable strategy. I never thought I would be actively promoting and discussing weight loss diets.”
But now he is, so, what’s to know about using Weiner’s ice diet?
When you eat a significant amount of ice, your body burns energy to melt it. Eating ice should, by the logic of this diet, also provide some level of satiety, if only so far as it physically fills space in the stomach and mouth.
By Weiner’s calculations, ingesting one liter of ice would burn about 160 calories, which is the energy equivalent of running one mile. So you get to eat and burn calories. Ever since the death of upward mobility, that has been The American Dream.
What’s more, it’s probably safe. “Ingesting ice at this level should not have any obvious adverse consequence in otherwise healthy persons,” Weiner, who trained at Johns Hopkins, writes. “For the vast majority of adults and children, there does not appear to be any contraindication to the use of the Ice Diet right now.”
One piece of evidence for the safety of ingesting substantial amounts of ice, Weiner notes, comes from the case study of the 32-ounce 7/11 Slurpee, from which he concludes, “The ingestion of one liter of ice per day appears to be generally safe.”
At some point beyond that liter, too much ice can be a problem. In the case of one obese person who attempted to eat seven quarts of ice per day, Weiner says, “Not surprisingly, this person suffered an uncomfortable feeling of coldness.” In his professional opinion, that much ice per day would, for most people, be a “toxic dose.” He recommends avoiding eating much more than the Slurpee-tested one liter of ice daily, “to avoid hypothermia or unusual cooling of the body. … Some organs do not work optimally when the body temperature drops too much.”
“For children using the Ice Diet, the amount of ice ingested should be monitored and related to their body weight and ability to report any problems that they might be having by ingesting ice.” Do not put ice into the mouths of children who can’t tell you if their brain has frozen.
For much the same reasons, use caution when using the ice diet during cold weather, Wiener says. Don’t eat ice on the ski slopes or while shoveling the walkway.
Don’t eat ice when you’re too hot, either. After running, for example, the body actually exerts energy through the active effort of dissipating excess heat that builds up during exercise. “If one were to ingest large amounts of ice as one was cooling off from exercise,” The Ice Diet warns, “some of the heat that had been generated by the exercise would be neutralized by the coolness of the ice, minimizing some of the energy burning benefits of the exercise.”
Physics writer Andrew Jones offers more skeptical calculations as to the caloric benefits of the ice diet, determining that eating a kilogram of ice would burn 117 calories. “To reach the 3,500 calories required to lose a pound of weight, it would be necessary to consume about 30 kilograms [66 pounds] of ice,” Jones writes. “Not exactly the most efficient diet plan.” That means, if you ate a liter of ice every day, you would lose about a pound of weight every month, all other things in life being equal. That’s not bad. And all other things wouldn’t be equal. Everything in your life would be different because you would be eating a liter of ice every day.
Also, of course, chewing ice can cause dental problems. Beyond full-blown cracking of teeth, the practice can damage the gums and enamel or injure the temporomandibular joint. To avoid dental damage, Weiner writes, “I would recommend that ice be allowed to melt in your mouth, as with ice pops, or consumed with the texture of shaved ice, as in the 7/11 Slurpee or the frozen margarita.”
Except don’t actually drink a liter of Slurpee every day because that sugar load would more than undermine this entire venture, and drinking a daily liter of margarita is this whole other thing. Weiner recommends making the process less onerous by making your own ice-pops using calorie free liquids instead of sugary concoctions or fruit juices. “For those with a larger budget, the Jimmy Buffett Margaritaville machine shaves ice into a very fine slurry, which can be consumed as-is or flavored with artificially flavored products.”
It’s that easy and, assuming the artificial flavoring you use is totally safe, you’re good to go. You don’t even have to worry about this fad diet becoming uncool. If anyone tells you it’s uncool, you can just cross your arms and say, “It’s objectively the coolest diet around in terms of temperature.” Pass the slurry.
If you’re sporting one of Fitbit’s activity trackers, you can now automate tasks and reminders with the help of IFTTT (If This Then That). The recipe-based software announced a dedicated channel for the sporty gadgets today, handling duties based on goals, activity, sleep, weight and more. For example, you can now log a weigh-in via text message or automatically beam sleep stats to a Google Spreadsheet each morning. Of course, those are just a couple of the possibilities, and users can construct their own formulas as well. Those who prefer Jawbone’s wearables have already been privy to the automated life logging, with other wrist-worn devices like the Pebble smartwatch supported too.
In response to last week’s Federal Budget, debate grows around whether or not the GST should be broadened to include fresh food. Calls are coming from MPs, former leaders and even the chief executive of World Vision Reverend Tim Costello, for an ‘adult conversation’ about a consumption tax on fresh fruit and vegetables. However, Australian research has shown a 10 per cent tax on fresh fruit and vegetables could have dire public health consequences.
Please leave your comments on this story below and if you’d like to have the program delivered weekly subscribe here.
Emeritus Professor Stephen Leeder AO – A Celebration!
Thursday, 1 May 2014 MacLaurin Hall, Quadrangle Building, University of Sydney
Colleagues gathered to celebrate the remarkable career of Emeritus Professor Stephen Leeder AO.
Keynote presentations and discussion focussed on the following themes: Chronic Disease: An international epidemic; Medical Education; Public Health Education and Training for the 21st Century; and Health Policy.