Well, your quantum computer is broken in every way possible simultaneously
Well, your quantum computer is broken in every way possible simultaneously
Not one stakeholder group left untrashed…
Great Einstein quote – the original definition of insanity presumably:
‘The significant problems we face cannot be solved at the same level of thinking we were at when we created them’
PDF: Braithwaite Delusions of health care JRSM 2014
The medical miracles delusion
Army ants subscribe to a simple rule: follow the ant
in front. If the group gets lost each ant tracks
another, eventually forming a circle. According to
crowd theorist James Surowiecki, one circle 400m
in circumference marched for two days until they
all died.1
Humans are not ants, but we often trudge together
along the same trail, neglecting to look around for
alternatives. Mass delusions involve large groups
holding false or exaggerated beliefs for sustained periods.
Humanity has a long, sorry list of these shadowthe-
leader epidemics of collective consciousness which
appear obviously wrong only in hindsight. Some last
for centuries: early alchemists intent on transmuting
base metals into gold and the Christian Crusades of
Europe’s middle ages, for example. Others have correlates
which resurface decades or centuries later:
McCarthy’s persecution of alleged communists in
the 1950s harked back to the Salem Witch hunts of
16th century America just as the 2008 Global
Financial Crisis had much in common with the
‘South Sea Bubble’ which slashed 17th century
Britain’s GDP.
In the educated 21st century, too, we blithely trust
in economic and political systems which are stripping
the earth’s resources, altering the climate and facilitating
wars. Are we then similarly mistaken, en masse,
about the capabilities of the health system?
Most of us believe in the miracles of modern medicine.
We like to think that the health system is
increasingly effective, that we are implementing
better treatments and cures with rapid diffusion of
new practices and pharmaceuticals and that there is
always another scientific or technological breakthrough
just around the corner promising to save
even more lives; all at an affordable price.
We maintain the faith despite multiple contraindications.
Modern health systems consistently deliver
at least 10% iatrogenic harm.2 Despite very large
investments and intermittent but important interventional
successes, such as checklists in theatres3 and
clinical bundles in ICU,4 there is no study showing
a step-change reduction in this rate, systems-wide.
Only half of care delivered is in line with guidelines,5
one-third is thought to be waste,6 and much is not
evidence-based,7 notwithstanding concerted efforts to
optimise that evidence and incorporate it into routine
practice.8
The reality is that progress is slowing, and medicine
seems to be reaching the limits of its capacities.
The potentially disastrous problems of antibiotic
resistance, for example, are yet to play out. This is
only one point among many. New technologies such
as the enormously expensive human genome project
have provided only marginal benefits to date. We still
do not have the answers to fundamental questions
about the causes of common diseases and how to
cure them. Many doctors are dissatisfied and increasingly
pessimistic.9,10 It must also be remembered that
although death is no longer seen as natural in the
modern era, everyone must die. Yet, we inflict most
of our medical ‘miracles’ on people during their last
six months of life. Le Fanu describes this levelling off
and now falling away of health care progress in The
Rise and Fall of Modern Medicine.11
Every major group of stakeholders has its own
specific delusion which acts to augment the metalevel
medical miracles delusion. Thus, the overarching
delusion is buttressed by a set of related ‘viruses
of the mind’, to borrow Richard Dawkins’ evocative
phrase.12
Although politicians think and act as if they are
running things, modern health systems are so complex
and encompass so many competing interests that no
one is actually in charge. Then, bureaucrats – acting
under their own brand of ‘groupthink’ – assume their
rules and pronouncements provide top-down stimulus
for medical progress and improved clinical performance
on the ground. Yet coalface clinicians are relatively
autonomous agents, so there can only ever be
modest policy trickle down.13,14
Researchers, too, support the medical miracles
industrial complex. The electronic database
PubMed holds some 23 million articles and is growing
rapidly. Every author hopes it will be his or her
results that will make a difference, yet there is far less
take up than imagined and comparatively little
investment in the science of implementation8 – translating
evidence into real life enhancements.
Nor are clinicians or the patients they serve
immune. While frontline clinicians strive to provide
good care, many myopically assume their practice is
above average; the so-called Dunning-Kruger
effect.15,16 Of course, statistically, half of all care clinicians
provide is below average. And notwithstanding
decades of public awareness, patients believe modern
medicine can repair them after decades of alcohol,
drugs, sedentary lives and dietary-excesses, despite
evidence to the contrary.
Meanwhile, the media’s unremitting propensity to
lend credibility to controversial views and to hone in
on ‘gee whiz’ breakthroughs – while ignoring the
incremental and the routine – fuels unrealistic expectations
of what modern medicine can deliver.
Throughout history, mass delusions have been
aligned with mass desires for favourable outcomes.
In the pursuit of medical miracles all of our interests
line up in a perfect circle. We seem more like army
ants than we think.
Just as the Global Financial Crisis was a wake-up
call for the serious consequences of blind fiscal faith
we must begin to manage our expectations of the
health system. Progress is always in jeopardy when
the real problems are obscured.
The challenge is to harness the tough-minded
scepticism needed to tackle this widely held ‘received
wisdom’. One realistic way forward is to encourage
stakeholders – politicians, policymakers, journalists,
researchers, clinicians, patients – to first consider
that their own and others’ perspectives are simply not
logically sustainable. This may be achieved through
genuine inter-group discourse about the health
system, where it is at, and its limitations.
As is so often the case, Albert Einstein said it best,
in a typically neat aphorism: ‘The significant problems
we face cannot be solved at the same level of
thinking we were at when we created them’.17 If we
can humbly accept that we need new perspectives
for healthcare – and radically different ways of
thinking – we will be better placed to free ourselves
from the hold of these peculiar viruses of the mind.
Andrew Ng on Deep Machine Learning via Large Scale Brain Simulation
https://www.youtube.com/watch?v=5elcmFNRCWk
The key determinants of learning accuracy are accessing as much data as possible and being able to process.
Partnered with the Google speech team.
Deep learning works well in two different settings:
1. Learning from labeled data > speech recognition, streetview images
2. Learning from unlabeled data >
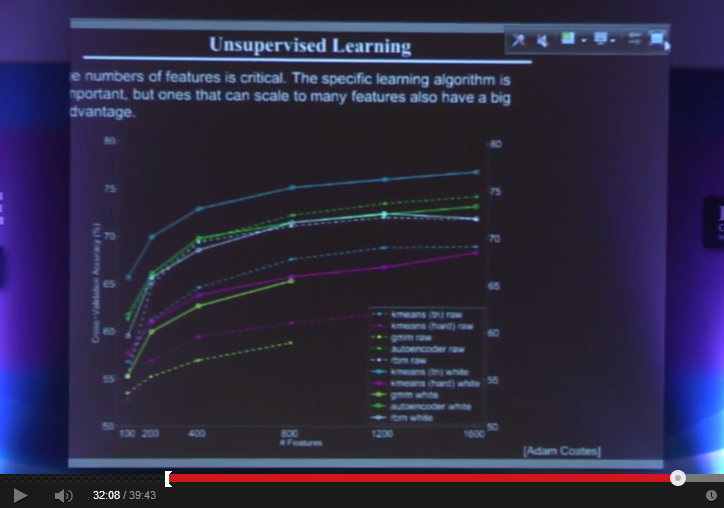
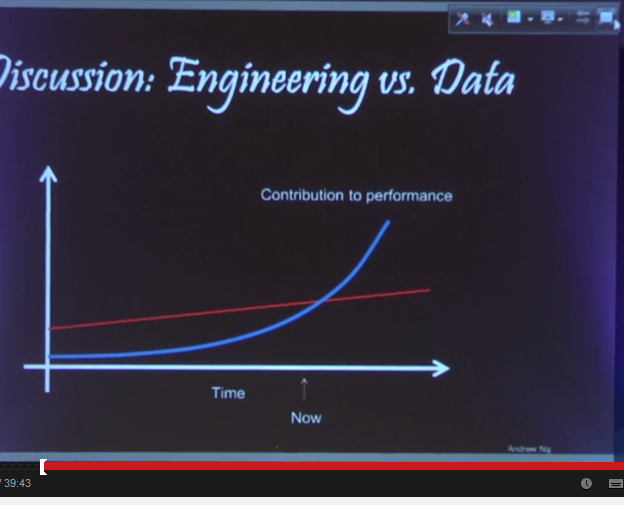
Up to now, humans have been driving performance due mainly to a lack of data and processing. With both of these now becoming available in abundance, machine learning will soon overtake human learning to become the dominant driver of performance.
Sky net.
Lissanthea put me on to this project.
Sounds highly aligned to my own ambitions, similarly requiring more focus…
http://www.wellthcare.com/
Wellthcare is an exploration
Health care contributes only 20% to our health and yet it dominates the health discourse;
80% of our health comes from our genes, behaviours, social factors and the environment
Wellthcare is about the 80%
It’s about finding new sources of health-related value
It’s about creating health
At Wellthcare we believe that much of this value resides in our networks and communities
We call this value Wellth
|
Recent Log posts
Pernicious moralising: when public health fails 22 Feb 2014 Wellthcare receives its first grant 6 Feb 2014 It’s time to prioritise health creation – not just care and prevention 30 Jan 2014 How a talking pet can keep us healthy 15 Jan 2014 Angelina Jolie, the end of standard, confused value, and not enough failure: why 2013 mattered 30 Dec 2013 Despatches from the Wellthcare Explorers Is there a role for an ‘event’? (PDF) Building Resilience: Understanding People’s Context and Assets (PDF) Fragmenting Communities and the Wantified Self (PDF) Discovering Wellth (PDF) |
Exploration timeline
Wellthcare is being explored by its Pioneer, Pritpal S Tamber, and an eclectic group of thinkers and doers called the Wellthcare Explorers. February 2014
January 2014
December 2013
November 2013
October 2013
September 2013
June 2013
May 2013
Feb 2013
|
Heart Foundation lays it all down… we need to lose a combined 120million KGs to return to normal healthy weight range… not as easy as it sounds.
http://www.medicalobserver.com.au/news/being-overweight-or-obese-now-the-norm

AUSTRALIANS need to lose a combined 120 million kilograms to return to a healthy weight range.
The average Australian man now weighs 85.9kg – that’s 6.5kg heavier than he was in 1989 – according to a National Heart Foundation analysis on the severity of the nation’s weight problem.
A breakdown of Heart Foundation national health surveys and government data also revealed that the average woman has gained 5.7kg in the past 25 years and now tips the scales at 71.1kg.
The Heart Foundation’s national director of cardiovascular health, Dr Rob Grenfell, said two-thirds of Australians now fall outside the healthy weight range, with nearly half a million people morbidly obese (BMI > 40).
“To return to a healthy weight range, an average man would need to lose 8.9kg and a woman would need to lose 5.7kg,” Dr Grenfell said.
“The combined weight loss required is just short of 120 million kilograms across the nation.”
The analysis highlights that the average BMI for men is up from 25.3 to 27.9 since 1989, and the average for women is up from 24.3 to 27.2.
Obesity has increased from 8.4% of the population in 1980, to 28.3% in 2011–12.
“It’s scary that two in three Australians are now above the healthy weight range, making overweight and obese weight ranges more ‘normal’ than healthy,” he said.
“The healthiest BMI is relatively lean, at around 22.5–24.9, which is equivalent to a weight of 70–77kg for an Australian man of average height and 59–65kg for an Australian woman of average height.”
In comparison to 1980, the proportion of obese adult Australians has tripled, while the number of people in the healthy weight range has almost halved.
WA and Queensland now have the highest average male BMIs at 28.2, according to the Australian Health Survey of 2011/12, with the highest average female BMIs, 27.7, occurring in SA and Tasmania.
Victoria has the lowest average BMIs at 27.6 for men and 26.9 for women.
Thanks Marion. Another book to chase up…

I spoke last night on a panel celebrating the release of this book. I gave it a rave blurb:
Lethal But Legal is a superb, magnificently written, courageous, and thoroughly compelling exposé of how corporations selling cigarettes, guns, cars, drugs, booze, and food and beverages enrich themselves at the expense of public health. Even more important, Freudenberg tells us how we can organize to counter corporate power and achieve a healthier and more sustainable environment. This book should be required reading for anyone who cares about promoting health, protecting democratic institutions, and achieving a more equitable and just society.
I will be using this one in classes. Congratulations to Nick Freudenberg, director of Hunter College’s Food Policy Center, for producing this distinguished work of scholarship.
Terrific summary of the state of play.
British gerontologist Aubrey de Grey believes achieving human immortality is inevitable. Last October de Grey told the audience at a US technology conference that they could expect to live 1000 years, maybe longer.
http://thenewdaily.com.au/life/2014/02/11/medical-science-close-curing-death/

Scientists are working to stop the ageing process, and extend the living… Photo: Shutterstock
Nanobots in your blood stream, backing up your brain to a computer, swapping your fallible human form for a sophisticated holographic avatar – it might sound like science fiction, but these are just some of the ways that science is hoping to extend human life and inch us closer to living forever.
US futurist, inventor and Google’s head of engineering, Ray Kurzweil has predicted that by the end of the century humans and machines will merge to create super humans who may never face the prospect of death. And Kurzweil, 65, hopes to be among those kicking mortality to the curb.

Ray Kurzweil: Working to bring an end to death. Photo: Getty
“Twenty years from now, we will be adding more time than is going by to your remaining life expectancy,” Kurzweil told Forbes Magazine. “We’ve quadrupled life expectancy in the past 1000 years and doubled it in the past 200 years. We’re now able to reprogram health and medicine as software, and so that pace is only going to continue to accelerate.”
Kurzweil is no slouch when it comes to accurate predictions. In the 1980s he predicted the incredible rise of the internet, foresaw the fall of the Soviet Union and identified the year when computers would beat humans at chess.
His next predictions include the programming of nanobots to work from within the body to augment the immune system and fight pathogens. By 2045 he sees us backing up our minds to the cloud and downloading ourselves into robotic forms.
And he’s not the only scientist hoping to blow out hundreds of candles in the future.
British gerontologist Aubrey de Grey believes achieving human immortality is inevitable. Last October de Grey told the audience at a US technology conference that they could expect to live 1000 years, maybe longer.
Ageing, he says, is a simple case of bad engineering, and once the human body’s kinks are ironed out we’ll be able to reverse its effects and put death on the back burner.
“My approach is to start from the straightforward principle that our body is a machine. A very complicated machine, but nonetheless a machine, and it can be subjected to maintenance and repair in the same way as a simple machine, like a car,” de Grey has said. “What I’m after is not living to 1000. I’m after letting people avoid death for as long as they want to.”
It’s a goal that even tech giant Google thinks is worth pursuing.
When Google entered the anti-ageing business last year, with the launch of its new biotechnology company Calico, it brought a new level of interest, respectability and crucially – funding – to the field.
Calico has poached some of the leading anti-ageing researchers from across the world to work on the challenge of extending life.
“I think that if Google succeeds, this would be their greatest gift to humanity,” said David Sinclair, an Australian professor of genetics at Harvard Medical School.
Professor Sinclair led a research team which last year announced it had reversed muscle ageing in mice, the results of which exceeded his expectations.
“We want immortality so badly that we’re always ready to be swept away into unthinkingness … Half in love with the impossible we’ve always wanted to conquer death.”
“I’ve been studying ageing at the molecular level now for nearly 20 years and I didn’t think I’d see a day when ageing could be reversed. I thought we’d be lucky to slow it down a little bit,” he was quoted as saying.
“There’s clearly much more work to be done here, but if those results stand, then aging may be a reversible condition, if it is caught early,” he said.
The research involved improving communication between a cell’s mitochondria and nucleus. Mitochondria are like a battery within a cell, powering important biological functions. When communication breaks down between this and the nucleus, the effects of ageing accelerate.
Human trials of the groundbreaking process are expected to start this year.
It’s the sort of breakthrough that can’t come soon enough for several billionaires across the globe who are pouring their fortunes and hopes into immortality research.
Russian entrepreneur, Dmitry Itskov founded the 2045 Initiative in 2011 with the aim of thwarting human death within three decades. Itskov envisages ‘neo-humans’ who will relinquish clunky human forms and adopt sophisticated machine bodies. He claims humans will eventually download their minds into artificial brains, which will then be connected to humanoid robots he calls Avatars.
According to 2045.com: “Substance independent minds will receive new bodies with capabilities far exceeding those of ordinary humans … Humanity will make a fully managed evolutionary transition and eventually become a new species.”
PayPal co-founder Peter Thiel donated $US3.5 million to Aubrey de Grey’s not-for-profit research foundation, telling the New Yorker at the time that: “Probably the most extreme form of inequality is between people who are alive and people who are dead”.
Clearly Thiel would prefer to remain among the living and he’s prepared to pay for his pitch at immortality, most recently making a large donation to the Singularity Institute, which focuses on creating artificial intelligence that could see the rise of cyborgs (merged humans and machines).
US entrepreneur turned science innovator, David Kekich, dedicated his life and impressive bank balance to reversing ageing after he was paralysed from a spinal cord injury in 1978. Kekich initially raised money for paralysis research but then switched to anti-ageing research. He founded the Maximum Life Foundation in 1999 and aims to reverse human ageing by 2033.
On his website Kekich writes: “We are moving from an era in which nothing could be done to defeat ageing into an era in which advancing biotechnology will give us the tools to do overcome it … Now, at the dawn of the biotechnology era, the inevitable is no longer inevitable. The research establishment – if sufficiently funded and motivated – could make spectacular inroads into repairing and preventing the root causes of ageing within our lifetime.”
But given that there are yet to be any proven means for extending human life, these billionaires may be motivated more by ego than altruism.
As US author Adam Leith Gollner writes in The Book of Immortality: the Science Belief and Magic Behind Living Forever (Sribner 2013): “We want immortality so badly that we’re always ready to be swept away into unthinkingness … Half in love with the impossible we’ve always wanted to conquer death.”
Yet he says all humans can really do to live longer is to eat well and exercise.
“We all have to go … whether dying in battle, tumbling off a horse, succumbing to pneumonia or being shivved by a lover. Maybe one day we just don’t wake up. However it happens, we enter the mystery.”
Lissanthea Taylor put me onto this conference that she was at:
PDF: Nudging-for-Better-Health-Conference-Flyer
Nudging for Better Health Conference

There is growing enthusiasm in government policy circles for promoting strategies designed to encourage and enable individuals to lead healthier lives. Such strategies draw on behavioural research showing individuals do not always act rationally and are susceptible to a range of influences which impact on the decisions they make. The research suggests that people can be nudged towards making decisions which are better for their health but in such a way that it does not unduly restrict their liberty or freedom to act.
This one-day conference will bring together an interdisciplinary group of scholars and commentators to explore the use of nudge strategies to incentivise better health. Recent developments in relation to the use of such strategies in Australia, NZ, the UK and Europe will be examined, as will case studies in specific areas impacting upon individual and collective health and wellbeing. The conference will be of interest to those working or researching in areas involving health and well being, and public health more generally.
Date: Monday, 17 February 2014
Time: 9am – 5pm
Venue: Monash University Law Chambers, 555 Lonsdale St Melbourne
Cost: Free
RSVP: Limited places are available. Please rsvp by Monday, 10 February, 2014 via e-mail toMeli.Voursoukis@monash.edu
Terrific Economist snippet…
http://www.economist.com/news/international/21595474-improve-health-care-governments-need-use-right-data-need-know

DECIDING where to seek treatment might seem simple for a German diagnosed with prostate cancer. The five-year survival rate hardly varies from one clinic to the next: all bunch around the national average of 94%. Health-care providers in Germany, and elsewhere, have usually been judged only by broad outcomes such as mortality.
But to patients, good health means more than life or death. Thanks to a study in 2011 by Germany’s biggest insurer, a sufferer now knows that the national average rate of severe erectile dysfunction a year after removal of a cancerous prostate gland is 76%—but at the best clinic, just 17%. For incontinence, the average is 43%; the best, 9%. But such information is the exception in Germany and elsewhere, not the rule.
Doctors and administrators have long argued that tracking patients after treatment would be too difficult and costly, and unfair to providers lumbered with particularly unhealthy patients. But better sharing of medical records and a switch to holding them electronically mean that such arguments are now moot. Risk-adjustment tools cut the chances that providers are judged on the quality of their patients, not their care.
In theory, national health-care systems should find measuring outcomes easier. Britain’s National Health Service (NHS) compiles masses of data. But it stores most data by region or clinic, and rarely tracks individual patients as they progress through treatment. Sweden’s quality registries do better. They analyse long-term outcomes for patients with similar conditions, or who have undergone the same treatment. Some go back to the 1970s and one of the oldest keeps records of hip replacements, letting medics compare the long-term performance of procedures and implants. Sweden now has the world’s lowest failure rate for artificial hips.
Elsewhere, individual hospitals are blazing a trail. Germany’s Martini-Klinik uses records going back a decade to fine-tune its treatment for prostate problems. The Cleveland Clinic, a non-profit outfit specialising in cardiac surgery, publishes a wide range of outcome statistics; it now has America’s lowest mortality rate for cardiac patients. And though American politicians flinch at the phrase “cost-effectiveness”, some of the country’s private health firms have become statistical whizzes. Kaiser Permanente, which operates in nine states and Washington, DC, pools the medical records for all its centres and, according to McKinsey, a consultancy, has improved care and saved $1 billion as a result.
Such approaches are easiest in fields such as prostate care and cardiac surgery, where measures for quality-of-life are clear. But some clinics have started to track less obvious variables too, such as how soon after surgery patients get back to work. This is new ground for doctors, who have long focused on clinical outcomes such as infection and re-admission rates. But by thinking about what matters to patients, providers can improve care and lower costs at the same time.
The 1 February edition of The Economist, in an article entitled Need to Know (about health outcomes), took up the theme. The article observed that in Germany, its biggest insurer made available data in 2011 about outcomes for all to see.
Among the outcomes, the data showed five-year survival after treatment for prostate cancer was uniform across the nation – 94 per cent. But the data collected by the insurer went further: while the national average for subsequent erectile dysfunction was 76 per cent, at the best-performing clinic it was just 17 per cent. “For incontinence, the average was 43 per cent: the best 9 per cent,” The Economist wrote.
Armed with data such as these, prospective patients can choose where to be treated. The same data form the basis for discussion between those who provide and those who pay for health care.
https://ama.com.au/ausmed/case-measuring-outcomes-what-we-do

Archie Cochrane, the Scottish medical epidemiologist after whom the Cochrane Collaboration that develops the evidence base for clinical medicine is named, came out of the Spanish Civil War and World War Two sceptical about the outcomes of his medical care.
Cochrane said, “I knew that there was no real evidence that anything we had to offer had any effect on tuberculosis, and I was afraid that I shortened the lives of some of my friends by unnecessary intervention.”
He changed career, moving into public health and conducting epidemiological research into TB and occupational lung diseases. He became especially sceptical about screening and, as Wikipedia puts it, “his ground-breaking paper on validation of medical screening procedures, published jointly with fellow epidemiologist Walter Holland in 1971, became a classic in the field”.
Cochrane recalled in his 1972 book Effectiveness and Efficiency: Random Reflections on Health Services being puzzled by a crematorium attendant he met who was permanently serenely happy. Cochrane asked why: the attendant said that each day he marvelled at seeing “so much go in and so little come out”. Cochrane suggested that he consider working in the National Health Service.
In Australia we assess how much work we do in hospitals through activity-based funding. Money flows in direct proportion – so many coronary grafts, so many strokes treated. But little attention, at least in routine care, is paid to what we achieve. There are examples that contradict this general assertion, but mainly it is true.
Recently, the Bureau of Health Information in the NSW Ministry of Health made available statewide mortality data for five conditions treated in NSW public hospitals, taking account of variations in severity. Such data begin to fill the blanks in our knowledge about outcomes, and prompt discussion about why these variations occur.
The 1 February edition of The Economist, in an article entitled Need to Know (about health outcomes), took up the theme. The article observed that in Germany, its biggest insurer made available data in 2011 about outcomes for all to see.
Among the outcomes, the data showed five-year survival after treatment for prostate cancer was uniform across the nation – 94 per cent. But the data collected by the insurer went further: while the national average for subsequent erectile dysfunction was 76 per cent, at the best-performing clinic it was just 17 per cent. “For incontinence, the average was 43 per cent: the best 9 per cent,” The Economist wrote.
Armed with data such as these, prospective patients can choose where to be treated. The same data form the basis for discussion between those who provide and those who pay for health care.
Once, clinical trials of new cancer drugs were concerned principally with the survival of patients treated versus those not treated with new medications. But they now measure more than life expectancy.
For over 25 years mortality data have been supplemented by quality of life assessments.
But the excellence in clinical trial outcome measurement has not spread to routine care.
So much goes in, but what comes out?
In the US, health care expenditure is a huge worry for individual citizens, for Government (which spends as much as a proportion of GDP/GNP as ours does on health), and for industry, which pays for a lot of health insurance for employees. In response, comparative effectiveness research – CER – has recently evolved.
Wikipedia advises that “The Institute of Medicine committee has defined CER as ‘the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, or to improve the delivery of care. The purpose of CER is to assist consumers, clinicians, purchasers, and policy makers to make informed decisions that will improve health care at both the individual and population levels’.”
There are many agencies and individuals now in the US committed to CER, including Dr John Wennberg at the Dartmouth Institute for Health Policy and Clinical Practice.
He and his colleagues have studied variations in medical practice across the US with a view to ironing out the wrinkles caused by inferior care.
They claim that 30 per cent of health care costs could be saved by correcting care that falls below expected outcomes.
Australia has not been entirely idle, and we have led the world in aspects of outcome measurement in relation to drugs.
Since 1953, Australia’s Pharmaceutical Benefits Advisory Committee (PBAC) has constructed the formulary of publicly funded medicines. Since 1990, the PBAC has made cost and effectiveness (outcome) assessment a mandatory prelude to listing. Pricing and other political decisions follow, but the solid outcome data are necessary. Others are now following our example.
When we have a health care system that is fully connected electronically, the task of measuring outcomes and using them to good effect in managing the system will be far easier. Outcome data are critical to achieving real financial efficiency. They can be used to help us stop doing things that achieve nothing, or cause harm, and instead use the resources saved for clinical care with good outcomes.
But assessing outcomes, as the prostate surgery example demonstrates, extends well beyond financial efficiency and, indeed, beyond life expectancy. When we confidently explain what we achieve with what we do – quantity and quality of life gained – patients are empowered to make choices.