http://www.economist.com/news/business/21595461-those-pouring-money-health-related-mobile-gadgets-and-apps-believe-they-can-work
WHEN Kenneth Treleani was told last summer that he was suffering from high blood pressure, his doctor prescribed medicine to tackle the condition. He also made another recommendation: that Mr Treleani invest in a wireless wrist monitor that takes his blood pressure at various times during the day and sends the data wirelessly to an app on his smartphone, which dispatches the readings to his physician. Mr Treleani says the device (pictured), made by a startup called iHealth, has already saved him several visits to the doctor’s surgery.
Portable blood-pressure monitors have been around for a while. But the idea of linking a tiny, wearable one to a smartphone and a software app is an example of how entrepreneurs are harnessing wireless technology to create innovative services. By letting doctors and carers monitor patients remotely, and by making it simpler to collect vast amounts of data on the effectiveness of treatments, the mobile-health industry, or m-health as it has become known, aims to drive down costs while improving results for patients.
Many experiments are already under way in emerging markets, where new mobile devices and apps are helping relieve pressure on poorly financed and ill-equipped clinics and hospitals. But the biggest prize is America, which splashes out a breathtaking $2.8 trillion each year on a health-care system riddled with inefficiencies. The prospect of revolutionising the way care is delivered there is inspiring entrepreneurs. Mercom Capital Group, a consulting firm, reckons that of the $2.2 billion venture capitalists put into health-care startups last year, mostly in America, $564m went to m-health businesses.
The m-health market can be broken down into two broad categories. First, there are the apps and appliances used to monitor the wearer’s physical fitness. Firms such as Nike, Fitbit and Jawbone make wristbands and other wearable gadgets full of sensors that let people record their performance, and their calorie-burning, as they pound the pavement or sweat in the gym.
Second, other apps and devices link patients with a medical condition to the health-care system. Last month Google said it was working on a contact lens containing a tiny wireless chip and sensors that would measure and transmit the glucose levels in a diabetic patient’s tears. In December Apple was granted an American patent on a means to incorporate a heartbeat sensor into its devices.
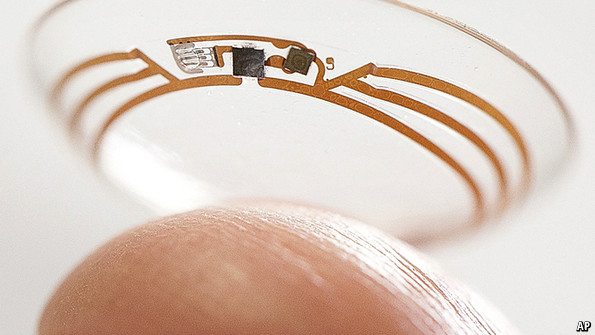
Keeping an eye on glucose levels
The fitness apps may help people to keep up their training regimes, and in time make the population healthier. But in the shorter term they will not have much effect on the health-care system. Nor may they make many investors rich. IMS Health, a research firm, says that of the 33,000-plus health-related apps on Google Play’s app store (the figure for Apple’s iTunes is over 43,000), just five of them—of which two are calorie-counters—account for 15% of all downloads.
A growing posse of entrepreneurs think the big money is to be made in the second category, of apps and devices that seek to transform the way health care is delivered. Large companies spy an opportunity here too. Qualcomm, which sells wireless technology and services, has set up an m-health division, Qualcomm Life, and built a technology platform to make it easy for m-health companies to combine data about things such as the medicines people take and the results of tests they run on themselves, so their doctors can get a more complete picture of their health.
Among those firms with products already for sale, AliveCor makes a $199 gadget that attaches to a smartphone and lets patients take an electrocardiogram by placing two fingers on metal plates. It also sells a veterinary version for taking pets’ ECGs. The data are displayed in an app on the phone and can be reviewed (for a fee) by a cardiologist. CellScope, another startup, makes an otoscope—a device for looking inside the ear—that can be attached to an iPhone and an app that can send the images it takes to a physician.
Last year Medtronic, a huge medical-devices company, splashed out $200m to buy Cardiocom, which combines telehealth services with wireless home gadgets, including scales for heart patients for whom sudden weight gain may be a dangerous symptom. In October Verizon, a mobile-telecoms operator, launched a platform to transmit data from home devices, such as glucose monitors, to the firm’s secure “cloud” of servers.
As Don Jones of Qualcomm Life puts is, just as a car’s electronics tell a driver about its condition, so m-health devices and apps “give people dashboards, gauges and alarm signals” that make it easier for them and their doctors to track what is happening with their bodies. This may alert them to the need for action well before the patient’s condition deteriorates to the extent that he needs hospital treatment. Given that in America the average cost of a night’s stay in hospital is almost $4,300, there is scope for significant savings.
Another obvious way to use the technology to avert health crises is by checking that patients are taking their medicines. Propeller Health sells a device that fits on top of asthma inhalers, to monitor their use. Proteus Digital Health, which raised $63m last year, is testing an ingestible sensor that is taken at the same time as prescribed medication. The device, which relies on stomach fluids to complete a circuit to power it, transmits information to a smartphone so doctors and carers can track when a patient takes pills.
Again, the goal is to save money while improving health. The average annual cost of, say, treating sufferers from high blood pressure who fail to take their medicines is nearly $4,000 more than the cost of treating those who pop their pills reliably.
If such products live up to their promise, a side-effect may be that there is less need for medical technicians—an example of a wave of technology-related job losses that some economists expect. The development of machine intelligence, another hot area for investment (see article), may eventually mean there is less need for doctors or specialists to analyse test results.
One snag is that techies’ enthusiasm for such innovation is colliding with the health-care industry’s conservatism. Doctors in America have been paid for delivering more care, so products that might lead to fewer billable patient visits are viewed with suspicion. This is changing gradually as insurers switch towards rewarding hospitals for providing a better quality of care instead of simply paying them for the quantity delivered. But there is a long way to go in making the medical profession take an interest in cost-saving: a study last month in Health Affairs, a journal, found that few American surgeons had any idea of the cost of the devices, such as replacement hip joints, they implant in patients.
Encouraging iPochondria
Insurers may have cause to worry that, instead of reducing doctors’ workloads, the spread of m-health devices and apps may only encourage hypochondria: surgeries may be flooded with the “worried well”, fussing over every slightly anomalous reading. That may keep the medical profession nicely busy, but will not curb the ever-rising cost of health care.
So, to win over doctors, hospital managers and insurers, m-health firms will need to gather evidence to support their claims of cost-cutting and improved patient outcomes. Such evidence is still surprisingly scarce, says Robert Kaplan of the National Institutes of Health, a government agency. Stephen Kraus of Bessemer Venture Partners, which has examined hundreds of m-health startups, says many firms are blithely assuming that all you have to do is “appify” health care and the world will change.
Makers of more sophisticated m-health products, aimed at doctors, clinics and hospitals rather than patients, will have to build a sales force like that of a pharmaceuticals company, says Bob Kocher of Venrock, another venture-capital firm. That will take time and lots of money.
Some m-health products may have to win approval from America’s Food and Drug Administration. Most firms were pleased by a plan the FDA published last year that said it would regulate only those m-health products that do the work of a traditional medical device—an ECG, say, but not a pedometer. But applying for approval is still burdensome. And the FDA has not finished drawing up its rules: m-health firms are waiting for a framework on the use of information technology in health care from the FDA and two other agencies. Despite such obstacles, optimists such as Peter Tippett of Verizon see health care undergoing the mobile transformation that banking and other industries have already been through.
Andrew Thompson, Proteus’s boss, hopes that the sensors and software his firm is developing will form the dominant “platform” for m-health in the way that Facebook dominates social networking and lets other firms build apps that run on it. But it is likely to face stiff opposition. Mr Kocher thinks giants like Google and Apple may seek to build m-health platforms too.
Apple filed its patent for a “seamlessly embedded heart-rate monitor” after looking for ways to replace passwords with biometric methods—in this case, an ECG—to authenticate users. It may think carefully before entering a business as heavily regulated as medical devices. But it has made no secret of its interest in selling wearable gadgets packed with sensors; and if consumers prove as keen on m-health as investors currently are, it will surely want to satisfy them.
Firms that aspire to make serious money in m-health will need plenty of patience and deep pockets. But they may be able to rely on an army of technophile patients who lobby their doctors to incorporate the new devices and apps in their treatment programmes. Mr Treleani is one of them: “I’d be suspicious of medical practices that aren’t moving forward with these new technologies,” he says.
 Smartphone app visualises two similar running routesI am obsessed with my running app. Last week obsession became frustration verging on throw-the-phone-on-the-floor anger. Wednesday’s lunchtime 5km run was pretty good, almost back up to pre-Christmas pace. On Friday, I thought I had smashed it. The first 2km were very close to my perennial 5 min/km barrier. And I was pretty sure I had kept up the pace. But the app disagreed.As I ate my 347 calorie salad – simultaneously musing on how French dressing could make up 144 of them – I switched furiously between the two running route analyses. This was just preposterous; the GPS signal must have been confused; I must have been held up overtaking that tourist group for longer than I realised; or perhaps the app is just useless and all previous improvements in pace were bogus.My desire to count stuff is easy to poke fun at. It’s probably pretty unhealthy too. But it’s only going to be encouraged over the next few years. Wearable technology is here to stay. Smart phone cameras
Smartphone app visualises two similar running routesI am obsessed with my running app. Last week obsession became frustration verging on throw-the-phone-on-the-floor anger. Wednesday’s lunchtime 5km run was pretty good, almost back up to pre-Christmas pace. On Friday, I thought I had smashed it. The first 2km were very close to my perennial 5 min/km barrier. And I was pretty sure I had kept up the pace. But the app disagreed.As I ate my 347 calorie salad – simultaneously musing on how French dressing could make up 144 of them – I switched furiously between the two running route analyses. This was just preposterous; the GPS signal must have been confused; I must have been held up overtaking that tourist group for longer than I realised; or perhaps the app is just useless and all previous improvements in pace were bogus.My desire to count stuff is easy to poke fun at. It’s probably pretty unhealthy too. But it’s only going to be encouraged over the next few years. Wearable technology is here to stay. Smart phone cameras 

")




