Nearly half of all Americans will get type 2 diabetes, says study
Type 2 diabetes, linked in 90% of cases to overweight and obesity, is soaring. New research shows 40% of Americans and 50% of Hispanics and non-Hispanic black women will get the disease at some point in their life and the numbers are unlikely to be much different elsewhere in the developed world
A patient undergoes a blood test for diabetes, a condition which brings icnreased risk of stroke and heart failure. Photograph: Hugo Philpott/PA
How much worse can the type 2 diabetes epidemic get? Shockingly, a new study published by a leading medical journal says that 40% of the adult population of the USA is expected to be diagnosed with the disease at some point in their lifetime. And among Hispanic men and women and non-Hispanic black women, the chances are even higher – one in two appear to be destined to get type 2 diabetes.
As Public Health England spelled out in a recent report urging local authorities to take action, 90% of people with type 2 diabetes are overweight or obese. There is no mystery behind the rise in diagnoses – they match the soaring weight of the population. The climb dates back to the 1980s and is associated with our more sedentary lifestyles and changing eating habits – more food, containing more calories, more often. It is those things that will have to be tackled if the epidemic is to be contained.
The new study in The Lancet Diabetes & Endocrinology journal, from a team of researchers from the Centers for Disease Control and Prevention in Atlanta, shows that the risk of developing type 2 diabetes for the average 20 year-old American rose from 20% for men and 27% for women in 1985–1989, to 40% for men and 39% for women in 2000–2011. The study was big – involving data including interviews and death certificates from 600,000 Americans.
Americans are generally living longer, which is a factor in their increased lifetime chance of developing type 2 diabetes. They are also not dying in the same proportions that they were, because of better treatment. However, that means they are going to spend far more years of their lives suffering from type 2 diabetes, which can lead to blindness and foot amputations as well as heart problems.
This is very bad news for the US healthcare system, says Dr Edward Gregg, study leader and chief of the epidemiology and statistics branch of the Division of Diabetes Translation at CDC:
As the number of diabetes cases continue to increase and patients live longer there will be a growing demand for health services and extensive costs. More effective lifestyle interventions are urgently needed to reduce the number of new cases in the USA and other developed nations.
Both he and Canada-based Dr Lorraine Lipscombe, who has written a commentary on the study, point out that the situation in the US is unlikely to be much different from that elsewhere in the developed world. Dr Lipscombe, from Women’s College Hospital and the University of Toronto, writes:
The trends reported by Gregg and colleagues are probably similar across the developed world, where large increases in diabetes prevalence in the past two decades have been reported.
Primary prevention strategies are urgently needed. Excellent evidence has shown that diabetes can be prevented with lifestyle changes. However, provision of these interventions on an individual basis might not be sustainable.
Only a population-based approach to prevention can address a problem of this magnitude. Prevention strategies should include optimisation of urban planning, food-marketing policies, and work and school environments that enable individuals to make healthier lifestyle choices. With an increased focus on interventions aimed at children and their families, there might still be time to change the fate of our future generations by lowering their risk of type 2 diabetes.
also discusses social determinants, and specifically the idea that less equal societies are comparatively less healthy across the board (including the wealthy)
The critical importance of poverty prevalence in a country’s health (AU is 12.5% c.f. average of 9% cf. US of 15%)
Woolf explained this disparity by citing the work of the British social epidemiologist Richard Wilkinson, who has proposed that income inequality generates adverse health effects even among the affluent. Wide gaps in income, Wilkinson argues, diminish our trust in others and our sense of community, producing, among other things, a tendency to underinvest in social infrastructure. Furthermore, Woolf told me, even wealthy Americans are not isolated from a lifestyle filled with oversized food portions, physical inactivity, and stress. Consider the example of paid parental leave, for which the United States ranks dead last among O.E.C.D. countries. It’s not hard to see how such policies might have implications for infant and child health.
Political systems have important effects on policy: fewer “choke points for special interests to block or reshape legislation,” such as filibusters or Presidential vetoes allows change to be enacted without extensive political negotiation.
Other countries have used their governments as instruments to improve health—including, but not limited to, the development of universal health insurance. Health-policy analysts have therefore considered the effect that different political systems have on public health. Most O.E.C.D. countries, for example, have parliamentary systems, where the party that wins the majority of seats in the legislature forms the government. Because of this overlap of the legislative and executive branches, parliamentary systems have fewer checks and balances—fewer of what Victor Fuchs, a health economist at Stanford, calls “choke points for special interests to block or reshape legislation,” such as filibusters or Presidential vetoes. In a parliamentary system, change can be enacted without extensive political negotiation—whereas the American system was designed, at least in part, to avoid the concentration of power that can produce such swift changes.
universal health coverage is not just altruistic, but also self-interested
healthcare is only responsible for between 10 and 25% of improvements in life expectancy – SDH responsible for the rest, mainly elements that impact on early childhood
Most experts estimate that modern medical care delivered to individual patients—such as physician and hospital treatments covered by health insurance—has only been responsible for between ten and twenty-five percent of the improvements in life expectancy over the last century. The rest has come from changes in the social determinants of health, particularly in early childhood.
Many Americans are aware that the United States spends much more on health care than any other country in the world. But fewer people know that the health of Americans—by many different measures—is actually worse than the health of citizens in other wealthy countries.Two major reports, both released last year, provide further elaboration of this apparent paradox. The first, “The State of US Health, 1990-2010,” documented trends in mortality and morbidity across the thirty-four member countries of the Organization for Economic Cooperation and Development (O.E.C.D.). The study, published in The Journal of the American Medical Association (to which I am a contributing writer), showed that both life expectancy and healthy-life expectancy improved in the United States over two decades. But the pace of those improvements was considerably slower in the United States: in 1990, the U.S. ranked twentieth among O.E.C.D. countries for life expectancy, and fourteenth for healthy-life expectancy; by 2010, it had fallen to twenty-seventh and twenty-sixth, respectively. The other charts and tables in the report—about heart, lung, and kidney disease; diabetes; injuries and homicides; depression; and drug abuse—all show Americans suffering poorer health.
The second report, commissioned by the National Institutes of Health, and conducted by the National Research Council (NRC) and the Institute of Medicine (IOM), convened a panel of experts to examine health indicators in seventeen high-income countries. It found the United States in a similarly poor position: American men had the lowest life expectancy, and American women the second-lowest. In some ways, these reports were not news. As early as the nineteen-seventies, a group of leading health analysts had noted the discrepancy between American health spending and outcomes in a book called “Doing Better and Feeling Worse: Health in the United States.” From this perspective, the U.S. has been doing something wrong for a long time. But, as the first of these two reports shows, the gap is widening; despite spending more than any other country, America ranks very poorly in international comparisons of health. The second report may provide an answer—supporting the intuition long held by researchers that social circumstances, especially income, have a significant effect on health outcomes.
Americans’ health disadvantage actually begins at birth: the U.S. has the highest rates of infant mortality among high-income countries, and ranks poorly on other indicators such as low birth weight. In fact, children born in the United States have a lower chance of surviving to the age of five than children born in any other wealthy nation—a fact that will almost certainly come as a shock to most Americans. But what causes such poor health outcomes among American children, and how can those outcomes be improved? Public-health experts focus on the “social determinants of health”—factors that shape people’s health beyond their lifestyle choices and medical treatments. These include education, income, job security, working conditions, early-childhood development, food insecurity, housing, and the social safety net.
Steven Schroeder, the former president of the Robert Wood Johnson Foundation—the largest philanthropic organization in the United States devoted to health issues—had a definitive answer to my question about why Americans might be less healthy than their developed-country counterparts. “Poverty,” he said. “The United States has proportionately more poor people, and the gap between rich and poor is widening.” Seventeen per cent of Americans live in poverty; the median figure for other O.E.C.D. countries is only nine percent. For three decades, America has had the highest rate of child poverty of any wealthy nation.
Steven Woolf, of Virginia Commonwealth University, who chaired the panel that produced the NRC-IOM report, also pointed to poverty when I asked him to explain the causes of America’s health disadvantage. “Could there possibly be a common thread that leads Americans to have higher rates of infant mortality, more deaths from car crashes and gun violence, more heart disease, more AIDS, and more premature deaths from drugs and alcohol? Is there some common denominator?” he asked. “One possibility is the way Americans, as a society, manage their affairs. Many Americans embrace rugged individualism and reject restrictions on behaviors that pose risks to health. There is less of a sense of solidarity, especially with vulnerable populations.” As a percentage of G.D.P., Woolf observed, the U.S. invests less than other wealthy countries in social programs like parental leave and early-childhood education, and there is strong resistance to paying taxes to finance such programs. The U.S. ranks first among O.E.C.D. countries in health-care expenditures, but as Elizabeth Bradley, a researcher at Yale, has documented, it ranks twenty-fifth in spending on social services.
The NRC-IOM report emphasized the effect of social forces on children and how those forces carry over to affect the health of adults, noting that American children are “more likely than children in peer countries to grow up in poverty” and that “poor social conditions during childhood precipitate a chain of adverse life events.” For example, of the seventeen wealthy democracies included in the report, the U.S. has the highest rates of adolescent pregnancy and sexually transmitted diseases, and the second-highest prevalence of H.I.V. This platform of adverse health influences in childhood sets up the health disadvantage that remains pervasive for all age groups under seventy-five in the United States.
It seems likely that many Americans would respond to these figures—and to the role poverty plays in poor health outcomes—by assuming that the data for all Americans is being skewed downward by the health of the poorest. That is, they understand that poor Americans have worse health, and presume that, because the United States has more poor people than other wealthy countries, the average health looks worse. But one of the most interesting findings in the NRC-IOM report is that even white, college-educated, high-income Americans with healthy behaviors have worse health than their counterparts in other wealthy countries.
Woolf explained this disparity by citing the work of the British social epidemiologist Richard Wilkinson, who has proposed that income inequality generates adverse health effects even among the affluent. Wide gaps in income, Wilkinson argues, diminish our trust in others and our sense of community, producing, among other things, a tendency to underinvest in social infrastructure. Furthermore, Woolf told me, even wealthy Americans are not isolated from a lifestyle filled with oversized food portions, physical inactivity, and stress. Consider the example of paid parental leave, for which the United States ranks dead last among O.E.C.D. countries. It’s not hard to see how such policies might have implications for infant and child health.
Other countries have used their governments as instruments to improve health—including, but not limited to, the development of universal health insurance. Health-policy analysts have therefore considered the effect that different political systems have on public health. Most O.E.C.D. countries, for example, have parliamentary systems, where the party that wins the majority of seats in the legislature forms the government. Because of this overlap of the legislative and executive branches, parliamentary systems have fewer checks and balances—fewer of what Victor Fuchs, a health economist at Stanford, calls “choke points for special interests to block or reshape legislation,” such as filibusters or Presidential vetoes. In a parliamentary system, change can be enacted without extensive political negotiation—whereas the American system was designed, at least in part, to avoid the concentration of power that can produce such swift changes.
Whatever the political obstacles, a major explanation for America’s persistent health disadvantage is simply a lack of public awareness. “Little is likely to happen until the American public is informed about this issue,” the authors of the NRC-IOM report noted. “Why don’t Americans know that children born here are less likely to reach the age of five than children born in other high income countries?” Woolf asked. I suggested that perhaps people believe that the problem is restricted to other people’s children. He said, “We are talking about their children and their health too.”
The superior health outcomes achieved by other wealthy countries demonstrate that Americans are—to use the language of negotiators—“leaving years of life on the table.” The causes of this problem are many: poverty, widening income disparity, underinvestment in social infrastructure, lack of health insurance coverage and access to health care. Expanding insurance coverage under the Affordable Care Act will help, but pouring more money into health care is not the only answer. Most experts estimate that modern medical care delivered to individual patients—such as physician and hospital treatments covered by health insurance—has only been responsible for between ten and twenty-five percent of the improvements in life expectancy over the last century. The rest has come from changes in the social determinants of health, particularly in early childhood.
Self-interest may be a natural human trait, but when it comes to public health other countries are showing the U.S. that what appears at first to be an altruistic concern for the health and care of the most vulnerable—especially children—may well result in improved health for all members of a society, including the affluent. Until Americans find their way to understanding this dynamic, and figure out how to mobilize public opinion in its favor, they will all continue to lose out on better health and longer lives.
Allan S. Detsky (M.D., Ph.D.) is a general internist and a professor of Health Policy Management and Evaluation and of Medicine at the University of Toronto, where he was formerly physician-in-chief at Mount Sinai Hospital. He is a contributing writer for The Journal of the American Medical Association.
From Forbes: http://www.forbes.com/sites/brucejapsen/2014/06/18/how-corporate-america-could-save-300-billion-by-measuring-health-like-financial-performance/
I write about health care and policies from the president’s hometown
6/18/2014 @ 11:00AM |2,724 views
How Corporate America Could Save $300 Billion By Measuring Health Like Financial Performance
The U.S. could save more than $300 billion annually if employers adopted strategies that promoted health, prevention of chronic disease and measured progress of “working-age” individuals like they did their financial performance, according to a new report.
The analysis, developed by some well-known public health advocates brought together and funded by The Vitality Institute, said employers could save $217 billion to $303 billion annually, or 5 to 7 percent of total U.S. annual health spending by 2023, by adopting strategies to help Americans head off “non-communicable” diseases like cancer, diabetes, cardiovascular and respiratory issues as well as mental health.
To improve, the report’s authors say companies should be reporting health metrics like BMI and other employee health statuses just like they regularly report earnings and how an increasing number of companies report sustainability. Corporations should be required to integrate health metrics into their annual reporting by 2025, the Vitality Institute said. A link to the entire report and its recommendations is here.
“Companies should consider the health of their employees as one of their greatest assets,” said Derek Yach, executive director of the Vitality Institute, a New York-based organization funded by South Africa’s largest health insurance company, Discovery Limited.
Those involved in the report say its recommendations come at a time the Affordable Care Act and employers emphasize wellness as a way to improve quality and reduce costs.
The Institute brought together a commission linked here that includes some executives from the health care industry and others who work in academia and business. Commissioners came from Microsoft (MSFT); the Robert Wood Johnson Foundation; drug and medical device giant Johnson & Johnson (JNJ); health insurer Humana (HUM); and the U.S. Department of Health and Humana Services.
The Vitality Institute said up to 80 percent of non-communicable diseases can be prevented through existing “evidence-based methods” and its report encourages the nation’s policymakers and legislative leaders to increase federal spending on prevention science at least 10 percent by 2017.
“Preventable chronic diseases such as lung cancer, diabetes and heart disease are forcing large numbers of people to exit the workforce prematurely due to their own poor health or to care for sick relatives,” said William Rosenzweig, chair of the Vitality Institute Commission and an executive at Physic Ventures, which invests in health and sustainability projects. “Yet private employers spend less than two percent of their total health budgets on prevention. This trend will stifle America’s economic growth for decades to come unless health is embraced as a core value in society.”
This means more people alive and less money spent on complications. We can squabble endlessly about how to define value in health care, but deaths avoided and dollars saved? That’s the real thing.
Recently, the Centers for Disease Control and Prevention (CDC) released data showing that health care–acquired infections (HAIs) are decreasing in the nation’s hospitals. Dropping fastest are central line–associated blood stream infections (44 percent from 2008–12) and some surgical site infections (down as much as 20 percent). This means more people alive and less money spent on complications. We can squabble endlessly about how to define value in health care, but deaths avoided and dollars saved? That’s the real thing.
Now the questions are: how did we accomplish this and how can we build on success? The credit flows in many directions.
Decades of scholarship have demonstrated the toll that medical mishaps, including preventable infections, take on patients; these avoidable complications cause tens of thousands of unnecessary deaths and injuries every year in U.S. hospitals. The 1999 Institute of Medicine report, To Err Is Human, was a landmark document that focused attention on patient safety, and thousands of studies since then have illuminated the specific problems that compromise patient safety and how to solve some of them.
Government research agencies, such as the Agency for Healthcare Research and Quality, funded many of these studies and have worked with private-sector groups, including hospital associations, the Institute for Healthcare Improvement, and a variety of regional improvement organizations and foundations to get the word out. Stakeholders hammered out valid, reliable, and widely accepted measures of infections that resulted in National Quality Forum–endorsed standards. The CDC has tracked infection rates, giving hospitals benchmarks against which to measure their own progress, and the Centers for Medicare and Medicaid Services has implemented new programs, established under the Affordable Care Act (ACA), that penalize hospitals with large numbers of preventable infections. The ACA also created a national network of hospitals to support improvements in patient safety.
The lesson: progress is possible when you have good scholarship documenting a really bad, solvable problem and then mobilize both the government and the private sector to take it on.
There is a lot more work to do. Some states are doing much better than others in tackling health care–acquired infections, as the infographic shows. Lagging states need to learn from leading ones. Progress is not uniform across the different types of infections. The number of catheter-associated urinary tract infections has actually increased slightly (3 percent).
But with so much to complain about in health care, we should take heart when science, government, and the private sector point the way toward a higher-performing health care system. And we should be realistic about what is required to maintain progress: we need government-supported scholarship to create a sound evidence base, private-sector leadership to implement new findings, and government regulations and incentives to spur that leadership on.
This morning, Apple made its much-anticipated move into healthcare with HealthKit (aka, the formerly rumored HealthBook.) With a typically dissonant and ever-growing ecosystem of health apps, devices and data, digital health needs a major player to enter to integrate these products and tools. We’re excited about what the largest company in the world is capable of doing for digital health. Here’s some perspective on what a seasoned digital health entrepreneur had to say about today.
Aaron Rowe
HealthKit is really exciting. Putting all of this information in one place, in a gorgeous app that will reach a ton of people, could do wonders for public health. But it won’t do much good if the on-screen content is designed without input from people who deeply understand health metrics. It looks like Apple or one of its partners made some technical mistakes on a slide that was shown during the big reveal of their new health app.
The slide, which appeared toward the end of the HealthKit segment of today’s WWDC keynote, neatly displays four key metrics for diabetes management: glucose, carbs, walking, and diabetes medication adherence. The numbers and units that Apple used as examples to illustrate their vision don’t make sense. When you measure your glucose with a personal blood sugar meter, it is measured in mg/dL— but the example shown by Apple displayed these numbers in mL/dL. Whoops!
What’s worse, the app screen features an SMS-style message from a particularly photogenic doctor who says, “You’re making great progress with your diet and exercise. Keep it up.” While the graph above this message shows a steady and very unhealthy looking uptrend in the users glucose readings. The current reading shown on the app is 122 “mL/dL”.
“People with a fasting glucose level of 100 to 125 mg/dL have impaired fasting glucose (IFG), or prediabetes,” according to a National Institute of Diabetes and Digestive and Kidney Diseases website. “A level of 126 mg/dL or above, confirmed by repeating the test on another day, means a person has diabetes.
It strikes me as particularly unusual that Apple would make these mistakes, since they are known for their intense attention to detail. Perhaps this kerfuffle happened because none of the folks who were involved with the WWDC keynote know what medical details should look like—is there some disconnect within the group that is building HealthKit? Have the designers who worked on this screen had enough contact with Apple’s partners at the Mayo Clinic or recently hired health experts? Not long ago, the Cupertino-based company onboarded several noninvasive glucose-monitoring experts from the wearable Raman spectrometer company C8 MediSensors and an early employee of Rock Health’s own Sano Intelligence.
I hope HealthKit will help patients understand and react to the results of every common blood test that is done in the home and medical labs–from cholesterol to creatinine. This could be one of the greatest ways in which Apple can make the world a better place. But they may need to sync internally to refine their understanding of these numbers, before they release this potentially lifesaving product into the wild.
Aaron Rowe is a research director at Integrated Plasmonics, a San Francisco startup that has developed a new class of spectrometer and surface plasmon resonance sensor chips. He and his colleagues are exploring ways to expand the scope of chronic disease management programs, enhance the success of new medications, and increase the usefulness of telemedicine by bringing a wide variety of in vitro diagnostics devices into the home and workplace. You can follow him on Twitter at @soychemist
Proteus occupy an interesting position… ingestibles are the ultimate in wearables. It’s smart also to be backed a big flailing incumbent player. It will be interesting to see if this stuff works.
Andrew Thompson on transforming healthcare at Wired Health 2014
Published On: May 5, 2014
Watch Proteus CEO Andrew Thompson present at Wired Health 2014 on transforming healthcare through digital medicines: http://bit.ly/1lS7RLe
WIRED Health is a one-day summit designed to introduce, explain and predict the coming trends facing the medical and personal healthcare industries. The inaugural event was held on Tuesday April 29, at the new home of the Royal College of General Practitioners, 30 Euston Square, London.
Research study results raise the question of whether some gastroenterologists do upper endoscopies to make money servicing Medicare beneficiaries who show no signs of illness on their first exam, Forbes reported. Often performed as an outpatient procedure, an upper endoscopy involves running a thin scope with a light and camera at its tip down the throat to check inside the upper digestive system for signs of serious illness. A study in the Annals of Internal Medicine analyzed data on almost 1 million randomly selected beneficiaries who had upper endoscopies between 2004 and 2006. Fifty-four percent of those who underwent the tests shouldn’t have had them, the study found. With the average cost of the procedure estimated at $3,000, the projected Medicare overpayment is $1.2 billion for 4 million unnecessary services performed nationwide during a three-year period, Forbes estimated.
Sometimes people flat out need cameras shoved down into their stomachs. A long history of reflux disease, for example, could prompt a gastroenterologist to perform an “upper endoscopy”—to run a thin tube down the patient’s throat in order to view their esophagus and stomach and look for signs of serious illness. Medicare has correctly decided that such upper endoscopies are valuable medical tests, and reimburse physicians relatively generously for performing them. But what should Medicare do when gastroenterologists unnecessarily repeat these tests in patients who do not show signs of serious illness on their first exam?
I became aware of this issue after reading an article in the Annals of Internal Medicine by Pohl and colleagues. Pohl glanced at billing data from a random sample of almost 1 million Medicare enrollees. (I am pleased with myself when I pull together a study of a few hundred patients. Perhaps I won’t be so pleased in the future.)
Pohl and colleagues analyzed how many patients received more than one upper endoscopy within a three year period. They then tried to figure out how often these repeat procedures were necessary, because of abnormalities discovered in the initial exam.
Let’s start with the bad news. Among those patients who should have received repeat tests, only half did so. That means even when doctors found bad things that needed to be followed up, it was practically a flip of a coin whether they would do so.
Now for the worse news. Among those who should not have received a follow-up test, a full 30% did, for a total of 20,000 such tests in this population. Here is a picture summarizing the results:
Here is another way to look at these results. Among patients receiving upper endoscopies, the majority –54%—should not have received these tests.
Now for some back-of-the-envelope math. The sample of patients Pohl and colleagues looked at made up 5% of the Medicare population. That means if you take their estimates of how many gastroenterologists performed unnecessary upper endoscopies over the three year period of their study, and multiply that estimate by 20, you end up with 4 million unnecessary endoscopies nationwide. With the average costs of such a procedure being around $3,000, that amounts to $1.2 billion of our tax dollars wasted on an unnecessary and, I should mention, uncomfortable and potentially harmful procedure. (Warning: I don’t know what Medicare pays for this test. But we are still talking hundreds of millions of dollars, in a best case scenario.)
In an editorial accompanying the Annals study, a gastroenterologist bemoaned these unnecessary procedures and recommended several steps we could take to reduce such testing. First, the editorialist said we should help physicians better understand when they should and should not use such procedures. Second, he said we “must also educate patients about the modest yield” of such tests.
I find this last idea…what’s a nice way to put this…highly naïve. (Haive?)
What we need to do is to stop paying doctors for unnecessary tests. Or alternatively, we need to pay doctors in ways that reduce their incentive to perform unnecessary tests, like lump sums to take care of all of their patients’ needs.
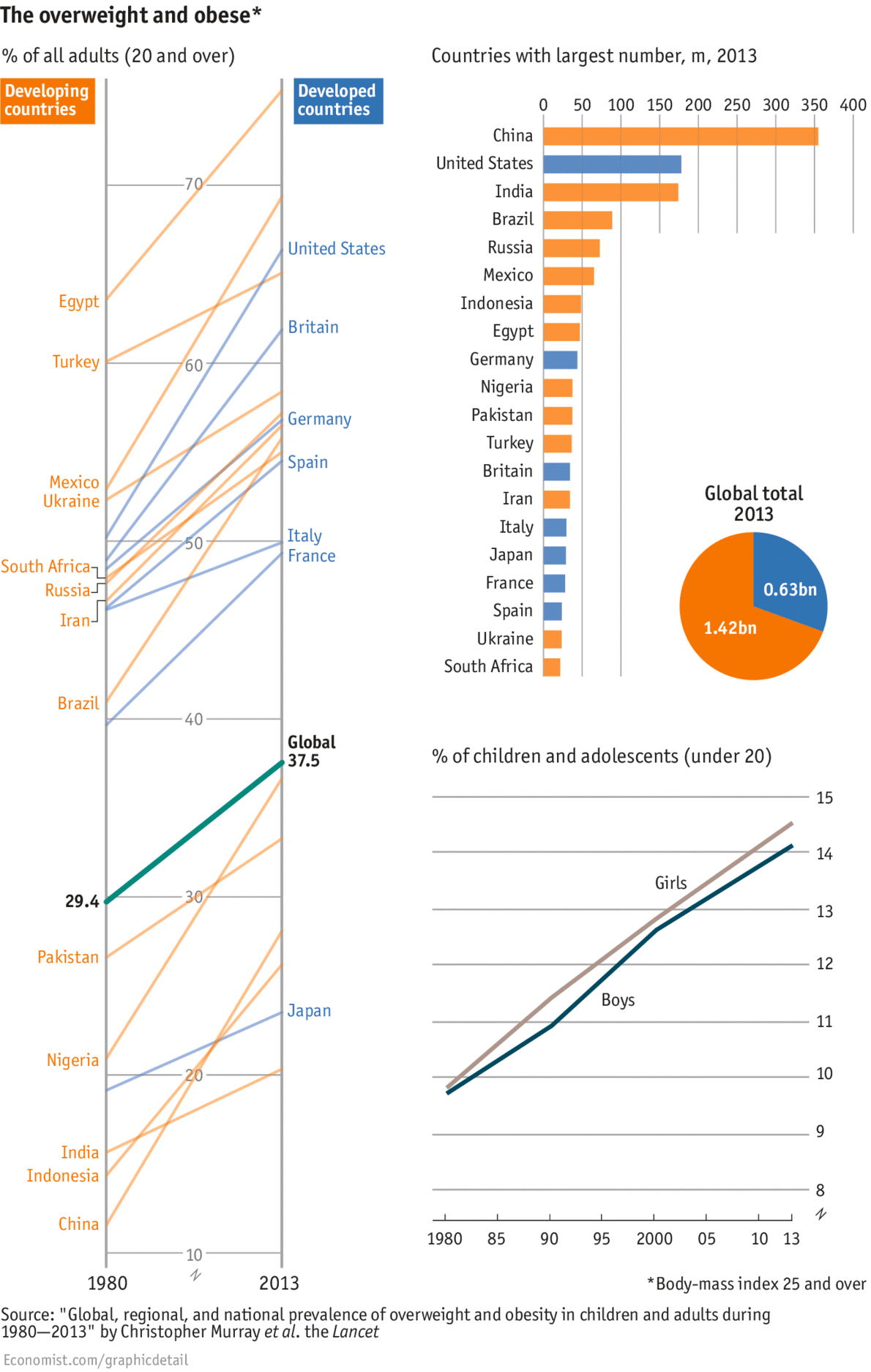
Worryingly, the study—led by the Institute of Health Metrics and Evaluation at the University of Washington—showed that children are fattening at a faster pace than adults. Last week the World Health Organisation set up a new commission to curb child obesity. But it will be some time yet before the world reaches peak fat.
WAISTLINES are widening everywhere. The percentage of adults who are overweight or obese has swelled from 29% in 1980 to 37% in 2013, according to a new study in the Lancet. People in virtually all nations got larger, with the biggest expansions seen in Africa, the Middle East and New Zealand and Australia. The chunkiest nations overall are found in the tiny Pacific islands and Kuwait, where over three-quarters of adults are overweight and over half are obese. And the world is unlikely to slim down soon. While the rate of increase has slowed in the rich world, it is still rising in poorer countries, where two-thirds of the world’s 2.1 billion overweight adults live. China is home to the largest number anywhere—335m, more than the population of America. This is not just because of its sheer size, but also because economic growth led to cellulite growth: a quarter of adults are now overweight compared with one in ten in 1980.Mexicans just outweigh neighbouring Americans. In both countries, two-thirds of people could lose a pound or two, though more Americans are obese. Agreeing on how to combat the problem is tricky, given that experts continue to bicker on what, precisely, makes us fat. Worryingly, the study—led by the Institute of Health Metrics and Evaluation at the University of Washington—showed that children are fattening at a faster pace than adults. Last week the World Health Organisation set up a new commission to curb child obesity. But it will be some time yet before the world reaches peak fat.
In response to last week’s Federal Budget, debate grows around whether or not the GST should be broadened to include fresh food. Calls are coming from MPs, former leaders and even the chief executive of World Vision Reverend Tim Costello, for an ‘adult conversation’ about a consumption tax on fresh fruit and vegetables. However, Australian research has shown a 10 per cent tax on fresh fruit and vegetables could have dire public health consequences.
Please leave your comments on this story below and if you’d like to have the program delivered weekly subscribe here.
We’re unlikely to solve persistent challenges to the health system, such as ensuring equitable access to well-coordinated care, with quick fixes. AAP Image/Quentin Jones
In the lead-up to the budget, the story of crisis has been hammered home, but there’s more to a country than its structural deficit. So how is Australia doing overall? In this special series, ten writers take a broader look at the State of Australia; our health, wealth, education, culture, environment, well-being and international standing.
In the lead up to this year’s federal budget, the government has been telling us short-term budget pain is needed to secure our long-term economic future.
The release of the National Commission of Audit report last week reinforced the government’s message that we need to do something more than tinker around the edges to get our economy back into shape.
But is Australia’s health system so bad it needs some kind of shock therapy to ensure it meets our future needs?
How are we doing now?
In 2011-12, Australia spent 9.5% of GDP on health, just higher than the OECD average of 9.3%. Twenty years ago, Australia spent 7.1% of GDP on health, which was about the OECD average. These figures somewhat undermine the argument that we have a crisis in health spending.
When you take a look at the headline indicator for health status, life expectancy, Australians are doing fairly well by global standards. In 2011, the average life expectancy for all Australians was 82 years, making us the seventh longest-living people among OECD nations.
There are some concerns, however, that we might not be living such long lives in the future. In 2011, Australians drank a little more alcohol than the OECD average (ten versus 9.3 litres per person per year). And we’re also a lot fatter: 21% of the population report being obese, compared with an OECD average of 15%.
While these indicators and global comparisons are useful high-level measures of our health system’s effectiveness, we need to get beyond averages to find the true picture.
Most people know – whether from personal experience or just watching the news – that our health system does not serve us all equally well. Some people cannot get access to essential health care, such as pharmaceuticals, general practitioners or dentists, when they need it simply because of cost.
Other people, especially those living in rural and remote areas, struggle to get access to services close to home.
And with some types of elective surgery and cancer services now predominately done in private hospitals, people without private health insurance can find themselves waiting for an excessively long time for treatment.
If the care you get depends to some extent on where you live, what you earn or whether or not you have private insurance, we have a problem with equitable access to care. And it’s a serious one too because there is strong evidence showing the people in most need of health care are the ones least able to afford it.
Getting timely access to care is one thing, but the quality of it matters too. In aninternational survey by the Commonwealth Fund, Australia’s performance was patchy on a series of quality measures.
When compared with seven other developed countries (including the United States, United Kingdom and New Zealand), Australia ranked sixth overall on a series measures looking at medical errors.
We ranked fourth on how well care was coordinated between different health professionals and third on how well care was centred around patient’s needs and preferences.
How we got here – past reforms
Medicare is the foundation of the Australian health system. The scheme, now 30 years old, is funded partly through our progressive tax system, and this is one of the key reasons our health system is considered to be relatively equitable. While Medicare has served us well, the time is right to consider reforms.
Medicare was originally developed to help people get access to basic medical and hospital care; in the 1960s when the scheme was conceived, most people suffered from relatively straightforward acute health conditions (infections, for instance, and traumatic injuries). Treatment from GPs, medical specialists and public hospitals was often all people needed to be cured.
Now, with more than seven million Australians having at least one chronic disease, people’s health needs are more complex. For some, a basic level of care might mean being treated by a GP, physiotherapist, dietitian, occupational therapist and an array of medical specialists. Medicare now funds a limited range of non-medical services, but much of what people need still falls outside its scope.
Medicare also works on an insurance model, with patients reimbursed for each visit to the doctor, and doctors paid largely on a fee-for-service basis. This model works reasonably well for one-off visits to the GP, but provides few incentives for health-care providers to work co-operatively and ensure patients receive coordinated care.
Over the last 20 years or so, federal and state governments have tried many different ways of improving the coordination of care. Some focused on reforms to financing health care, for example, the coordinated care trials of the 1990s.
Others have tried to improve coordination by making changes to the governance of the health system at the local level – the more recent establishment of Medicare Locals is an example.
In some areas, the long struggle to improve the coordination of care is starting to pay off, but these successes have yet to be replicated cross the country.
What’s next?
The National Commission of Audit report recommended some major changes to the structure and operation of our health system, and a 12-month period to review some of the proposals it outlined. But before the government looks at them in any detail, it’s important to recognise the limits of what Medicare, or any health system, can do to improve the length and quality of people’s lives.
It is well established that health services are just one of many factors that influence health outcomes. Other important determinants of health include the social, economic and physical environment, and people’s individual characteristics and behaviours. To improve the health of Australians, governments will also need to make gains in some of these other areas that determine health outcomes.
Health systems, however, do have an influence on health outcomes. A large study of 136 countries found that there was a correlation between rates of death and certain health system variables. Countries with more doctors, lower out-of-pocket costs, and higher total expenditure, for example, had lower premature death rates at the national level.
When you take a look at the headline indicator for health status, life expectancy, Australians are doing fairly well.Mercy Health/Flickr, CC BY-NC-ND
While this study includes many less wealthy countries than Australia, it shows that the design and operation of our health system does matter, even to headline indicators such as mortality.
The Australian health system clearly has some problems that need to be addressed, but they are long-standing ones, and ones shared by most other OECD countries.
We are unlikely to solve persistent challenges, such as ensuring equitable access to well-coordinated care, with quick fixes (we have tried most of them before). Nor are they likely to be solved by reforms naïvely borne out of economic theory, or imported holus bolus from other countries.
To improve Australia’s health system, we need to carefully consider a range of reforms and evaluate their potential to solve the most important problems we face (and this is not overall health expenditure).
If we don’t, we will simply add to the growing pile of overly ambitious reform proposals that have fallen by the wayside and made no difference at all.