Dr Paul Zollinger-Read is Chief Medical Officer at Bupa
He’s tried to think about the future
ubiquitous, embedded sensors will be important
gamification will help change behaviours
In November 2013, Bupa signed a partnership agreement with the United Nations agency, the International Telecommunication Union (ITU), to work together on a global ‘m-Health’ initiative called ‘Be Healthy, Be Mobile’.
By 2024, mobile technology will have completely transformed medical provision across the world, according to global healthcare company Bupa. Clothes, household appliances and furniture will all play a vital role behind the scenes of our daily routines, helping keep track of health and alerting people at the first sign of illness.
Meanwhile, ‘gamification’ of healthcare could reward everyday positive choices and healthy behaviour in the same way gamers unlock badges in mobile apps such as Angry Birds or Foursquare, aiding disease prevention and dramatically reducing the onset of diseases such as diabetes.
“This glimpse into the future has allowed us to imagine a time where sophisticated mobile technology and advancements in the connected home mean that people can become guardians of their own health,” said Dr Paul Zollinger-Read, Chief Medical Officer at Bupa.
“Being aware of their likelihood of disease and possible risk factors, coupled with constant monitoring through intelligent technology means that they will be able to spot the symptoms of illness from a very early stage, or simply prevent them altogether.”
Some of the innovative healthcare solutions suggested by Bupa include ‘smart’ nappies that allow parents to check their child’s hydration levels or monitor for kidney infections, intelligent fibres in clothing that canl detect movement of the chest and pulse, monitoring breathing and heart rate and detecting irregularities, and contact lenses featuring microscopic cameras that will monitor changes in the back of the eye, spotting early signs of diabetes.
Shoes featuring pressure sensors could detect when the wearer is sedentary, and alert them with updates on fitness goals, and the household fridge will monitor liquid, nutrition and calorie consumption, while ‘tattoo’ skin patches will monitor body temperature and hydration.
Bupa said that wearable technology and the connected home will transform prevention of diseases in the next decade by gathering data from a number of devices about our bodies and presenting it back to us in simple, visual, practical terms.
The news comes after Google unveiled a revolutionary smart contact lens which detects glucose levels in diabetes sufferers’ tears earlier this year. Human trials of a miniature artificial pancreas are also set to begin in 2016.
In November 2013, Bupa signed a partnership agreement with the United Nations agency, the International Telecommunication Union (ITU), to work together on a global ‘m-Health’ initiative called ‘Be Healthy, Be Mobile’.
Bupa and ITU will provide multidisciplinary expertise, health information and mobile technology to fight chronic diseases including diabetes, cancer, cardiovascular and chronic respiratory diseases, in low- and middle-income countries.
There is growing enthusiasm in government policy circles for promoting strategies designed to encourage and enable individuals to lead healthier lives. Such strategies draw on behavioural research showing individuals do not always act rationally and are susceptible to a range of influences which impact on the decisions they make. The research suggests that people can be nudged towards making decisions which are better for their health but in such a way that it does not unduly restrict their liberty or freedom to act.
This one-day conference will bring together an interdisciplinary group of scholars and commentators to explore the use of nudge strategies to incentivise better health. Recent developments in relation to the use of such strategies in Australia, NZ, the UK and Europe will be examined, as will case studies in specific areas impacting upon individual and collective health and wellbeing. The conference will be of interest to those working or researching in areas involving health and well being, and public health more generally.
Presenters
Dr Rory Gallagher & Mr Simon Raadsma, Behavioural Insights Team, NSW Department of Premier and Cabinet
Professor Christine Parker, Monash Centre for Regulatory Studies
Assoc. Professor Anne-Maree Farrell, Faculty of Law, Monash University
Assoc. Professor Duncan Mortimer, Centre for Health Economics, Monash University
Professor Michael Selgelid, Director, Centre for Human Bioethics, Monash University
Dr Liam Smith, Director, BehaviourWorks, Monash Sustainability Institute
Ms Jane Martin, Cancer Council Victoria
Ms Sondra Davoren, McCabe Centre for Law and Cancer
Dr Muireann Quigley, Bristol University, UK
Dr Elen Stokes, Cardiff University, UK
Dr John Kennelly, University of Auckland, NZ
Ms Paula O’Brien, Melbourne Law School
Event details
Date: Monday, 17 February 2014
Time: 9am – 5pm
Venue: Monash University Law Chambers, 555 Lonsdale St Melbourne
Cost: Free
RSVP: Limited places are available. Please rsvp by Monday, 10 February, 2014 via e-mail toMeli.Voursoukis@monash.edu
To improve health care, governments need to use the right data
DECIDING where to seek treatment might seem simple for a German diagnosed with prostate cancer. The five-year survival rate hardly varies from one clinic to the next: all bunch around the national average of 94%. Health-care providers in Germany, and elsewhere, have usually been judged only by broad outcomes such as mortality.
But to patients, good health means more than life or death. Thanks to a study in 2011 by Germany’s biggest insurer, a sufferer now knows that the national average rate of severe erectile dysfunction a year after removal of a cancerous prostate gland is 76%—but at the best clinic, just 17%. For incontinence, the average is 43%; the best, 9%. But such information is the exception in Germany and elsewhere, not the rule.
Doctors and administrators have long argued that tracking patients after treatment would be too difficult and costly, and unfair to providers lumbered with particularly unhealthy patients. But better sharing of medical records and a switch to holding them electronically mean that such arguments are now moot. Risk-adjustment tools cut the chances that providers are judged on the quality of their patients, not their care.
In theory, national health-care systems should find measuring outcomes easier. Britain’s National Health Service (NHS) compiles masses of data. But it stores most data by region or clinic, and rarely tracks individual patients as they progress through treatment. Sweden’s quality registries do better. They analyse long-term outcomes for patients with similar conditions, or who have undergone the same treatment. Some go back to the 1970s and one of the oldest keeps records of hip replacements, letting medics compare the long-term performance of procedures and implants. Sweden now has the world’s lowest failure rate for artificial hips.
Elsewhere, individual hospitals are blazing a trail. Germany’s Martini-Klinik uses records going back a decade to fine-tune its treatment for prostate problems. The Cleveland Clinic, a non-profit outfit specialising in cardiac surgery, publishes a wide range of outcome statistics; it now has America’s lowest mortality rate for cardiac patients. And though American politicians flinch at the phrase “cost-effectiveness”, some of the country’s private health firms have become statistical whizzes. Kaiser Permanente, which operates in nine states and Washington, DC, pools the medical records for all its centres and, according to McKinsey, a consultancy, has improved care and saved $1 billion as a result.
Such approaches are easiest in fields such as prostate care and cardiac surgery, where measures for quality-of-life are clear. But some clinics have started to track less obvious variables too, such as how soon after surgery patients get back to work. This is new ground for doctors, who have long focused on clinical outcomes such as infection and re-admission rates. But by thinking about what matters to patients, providers can improve care and lower costs at the same time.
The 1 February edition of The Economist, in an article entitled Need to Know (about health outcomes), took up the theme. The article observed that in Germany, its biggest insurer made available data in 2011 about outcomes for all to see.
Among the outcomes, the data showed five-year survival after treatment for prostate cancer was uniform across the nation – 94 per cent. But the data collected by the insurer went further: while the national average for subsequent erectile dysfunction was 76 per cent, at the best-performing clinic it was just 17 per cent. “For incontinence, the average was 43 per cent: the best 9 per cent,” The Economist wrote.
Armed with data such as these, prospective patients can choose where to be treated. The same data form the basis for discussion between those who provide and those who pay for health care.
Archie Cochrane, the Scottish medical epidemiologist after whom the Cochrane Collaboration that develops the evidence base for clinical medicine is named, came out of the Spanish Civil War and World War Two sceptical about the outcomes of his medical care.
Cochrane said, “I knew that there was no real evidence that anything we had to offer had any effect on tuberculosis, and I was afraid that I shortened the lives of some of my friends by unnecessary intervention.”
He changed career, moving into public health and conducting epidemiological research into TB and occupational lung diseases. He became especially sceptical about screening and, as Wikipedia puts it, “his ground-breaking paper on validation of medical screening procedures, published jointly with fellow epidemiologist Walter Holland in 1971, became a classic in the field”.
Cochrane recalled in his 1972 book Effectiveness and Efficiency: Random Reflections on Health Services being puzzled by a crematorium attendant he met who was permanently serenely happy. Cochrane asked why: the attendant said that each day he marvelled at seeing “so much go in and so little come out”. Cochrane suggested that he consider working in the National Health Service.
In Australia we assess how much work we do in hospitals through activity-based funding. Money flows in direct proportion – so many coronary grafts, so many strokes treated. But little attention, at least in routine care, is paid to what we achieve. There are examples that contradict this general assertion, but mainly it is true.
Recently, the Bureau of Health Information in the NSW Ministry of Health made available statewide mortality data for five conditions treated in NSW public hospitals, taking account of variations in severity. Such data begin to fill the blanks in our knowledge about outcomes, and prompt discussion about why these variations occur.
The 1 February edition of The Economist, in an article entitled Need to Know (about health outcomes), took up the theme. The article observed that in Germany, its biggest insurer made available data in 2011 about outcomes for all to see.
Among the outcomes, the data showed five-year survival after treatment for prostate cancer was uniform across the nation – 94 per cent. But the data collected by the insurer went further: while the national average for subsequent erectile dysfunction was 76 per cent, at the best-performing clinic it was just 17 per cent. “For incontinence, the average was 43 per cent: the best 9 per cent,” The Economist wrote.
Armed with data such as these, prospective patients can choose where to be treated. The same data form the basis for discussion between those who provide and those who pay for health care.
Once, clinical trials of new cancer drugs were concerned principally with the survival of patients treated versus those not treated with new medications. But they now measure more than life expectancy.
For over 25 years mortality data have been supplemented by quality of life assessments.
But the excellence in clinical trial outcome measurement has not spread to routine care.
So much goes in, but what comes out?
In the US, health care expenditure is a huge worry for individual citizens, for Government (which spends as much as a proportion of GDP/GNP as ours does on health), and for industry, which pays for a lot of health insurance for employees. In response, comparative effectiveness research – CER – has recently evolved.
Wikipedia advises that “The Institute of Medicine committee has defined CER as ‘the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, or to improve the delivery of care. The purpose of CER is to assist consumers, clinicians, purchasers, and policy makers to make informed decisions that will improve health care at both the individual and population levels’.”
There are many agencies and individuals now in the US committed to CER, including Dr John Wennberg at the Dartmouth Institute for Health Policy and Clinical Practice.
He and his colleagues have studied variations in medical practice across the US with a view to ironing out the wrinkles caused by inferior care.
They claim that 30 per cent of health care costs could be saved by correcting care that falls below expected outcomes.
Australia has not been entirely idle, and we have led the world in aspects of outcome measurement in relation to drugs.
Since 1953, Australia’s Pharmaceutical Benefits Advisory Committee (PBAC) has constructed the formulary of publicly funded medicines. Since 1990, the PBAC has made cost and effectiveness (outcome) assessment a mandatory prelude to listing. Pricing and other political decisions follow, but the solid outcome data are necessary. Others are now following our example.
When we have a health care system that is fully connected electronically, the task of measuring outcomes and using them to good effect in managing the system will be far easier. Outcome data are critical to achieving real financial efficiency. They can be used to help us stop doing things that achieve nothing, or cause harm, and instead use the resources saved for clinical care with good outcomes.
But assessing outcomes, as the prostate surgery example demonstrates, extends well beyond financial efficiency and, indeed, beyond life expectancy. When we confidently explain what we achieve with what we do – quantity and quality of life gained – patients are empowered to make choices.
Jawbone, maker of the UP fitness tracker bangle (and apparently not the company in Google’s Glassy sights), is running sweat-free towards an IPO. Action camera maker GoPro — ok, not technically a wearables company but the point of its cameras are that they are, y’know, wearable — has already filed for one. Smartwatch maker Pebble has raised a tonne of money since 2012, first via Kickstarter and then, off the back of its snowballing crowdfunder, from VC checkbooks.
Even though the genuine usefulness of bits of technology that you strap to your person still has a lot of proving to do – vs the intrusion (both visual, with a lot of these early devices being best described as uuuuuuuugggglllyyy; and, more importantly, the sensitive personal data being captured and monetized) – it’s the big huge lucrative potential that’s exciting makers and investors.
Mature Western markets are saturated with smartphones — ergo step forward sensor-stuffed wearables as the next growth engine for device makers. Devices whose literal positioning on our bodies enables them to gather far more intimate data on the lives and (physical) habits of users than previous generations of consumer mobiles. If only we can be persuaded to wear this stuff.
Yesterday analyst Canalys suggested 2014 will be the year for the wearables category becomes a “key consumer technology” — with more than 17 million wearable bands (alone) forecast to ship this year, rising to 23 million by 2015, and more than 45 million by 2017.
So that’s only wearable tech targeting the wrist, such as the Fitbit fitness tracker and Samsung’s Galaxy Gear smartwatch — it does not include devices aiming to squat on other body-parts (such as Google Glass). In short: tech makers gonna put a smart ring on it. Many are already trying.
On the ‘who is already making what’ front, wearable tech research and consulting firm Vandrico has put together this neat overview of the space — tracking the number of devices in existence; areas of market focus; and even which parts of the body are being targeted most.
(The most popular anatomical target for wearables is the wrists, since you’re curious — with 56 devices vying for that small patch of flesh; followed by the head, with 34 devices wanting to cling to it. On the flip side, the least popular body part for wearables thus far is apparently the hand, with just two devices listed, although the data doesn’t delve into the crotch region, so, yeah, there’s there too. Makers apparently not falling over themselves to fashion iCodpieces…).
According to Vandrico, there are some 115 wearables in play already; with an average selling price of $431; and with lifestyle, fitness and medical being the most popular market areas targeted (in that order).
The researcher has also taken the time to list and profile every single one of the 115 wearables it reckons are currently in play, so you don’t have to — from 3L Labs Footlogger to the ZTE Bluewatch (another mobile maker doing a smartwatch, who knew?).
Or at least all of the wearables its research has turned up. It’s asking for submissions for missing devices so it can keep expanding this database. (I’m going to throw the Fin into the ring on that front.)
Click here to check out — and start quantifying — the data for yourself.
How Would You Feel About Your Government Texting You To Tell You To Exercise?
A few overweight residents of this U.K. town are about to find out.
“Maybe walk to the shops or take the stairs more often.” “Aim to eat regular meals and keep a check on snacks and drinks.” “Eat fruit and veg.” These are some of the texts you get when you sign up for a new health program. The sender? The U.K. city of Stoke-on-Trent.
Stoke is starting the controversial project because it reckons that regular reminders are key to changing habits, and because getting people to slim down helps public budgets. “This is all about getting people on board and taking action before they need medical support, which is so expensive and personally upsetting,” a spokesperson told the BBC.
The British public hasn’t been so positive, though. Twitter lit up after the scheme was reported, with many bemoaning the long arm of government and wasted public money. Others said the texts could backfire, giving people a negative self-image (though presumably if they sign up in the first place, they’re not feeling good about themselves).
The program, which runs for 10 weeks, costs $16,000 to taxpayers, including set-up charges. About 500 people will participate voluntarily, all of them above the overweight limit, with a body mass index above 25. Officials say $16,000 is a pittance against the cost of treating obesity-related diseases.
Time will tell if the texts work. Other similar experiments show that it might, if people want to be involved and aren’t forced into anything.
Predictive analytics is “powered by the world’s most potent, booming unnatural resource: data.”
You have been predicted — by companies, governments, law enforcement, hospitals, and universities. Their computers say, “I knew you were going to do that!”
We are better than ever at making predictions – whether you’re going to click, lie, buy or die, as Eric Siegel puts it.
In a lesson on Big Think Edge, the only forum on YouTube designed to help you get the skills you need to be successful in a rapidly changing world, Siegel, a former professor at Columbia University, shows how predictive analytics is “powered by the world’s most potent, booming unnatural resource: data.”
You have been predicted — by companies, governments, law enforcement, hospitals, and universities. Their computers say, “I knew you were going to do that!”
Advertising
Netflix and Pandora predict the movies and music you will like. Online dating sites select possible matches for you based on your interests. Companies can predict whether you’re going to default on your credit card statements and whether you’re going to commit an act of fraud.
So what do governments and companies do with this gold mine? In the video below, Siegel tells Big Think that these entities not only have the power to predict the future “but also to influence the future.” And so can you.
Sign up for a free trial subscription on Big Think Edge and watch Siegel’s lesson here:
https://www.youtube.com/watch?v=Kriiamz9KqQ
Reflection Questions
— Describe how your company is using predictive analytics to influence any operational decisions? Do you analyze who is likely to respond before initiating a marketing campaign? If not, how could this help streamline operations in your department?– How are predictive analytics at work in your life? Do you use Netflix or Pandora to predict movies or music you will like? Have you used an online dating site that selects possible matches for you based on your interests? How has this worked out for you?
— Is the use of predictive analysis exposing people to other people, entertainment, or services that more accurately match their interests or is it pigeonholing people by suggesting things they may like based only on a limited amount of information on previous decisions they’ve made?
For expert video content to inspire, engage and motivate your employees, visit Big Think Edge.
Watch the video below and sign up for your free trial to Big Think Edge today.
Those respondents who had been and remained physically active aged most successfully, with the lowest incidence of major chronic diseases, memory loss and physical disability. But those people who became active in middle-age after having been sedentary in prior years, about 9 percent of the total, aged almost as successfully. These late-in-life exercisers had about a seven-fold reduction in their risk of becoming ill or infirm after eight years compared with those who became or remained sedentary, even when the researchers took into account smoking, wealth and other factors.
Exercise confers a reduction in mortality approximately the same as smoking cessation.
successful aging involves minimal debility past the age of 65 with little or no serious chronic disease diagnoses, depression, cognitive decline or physical infirmities that would prevent someone living independently
several, unsurprising factors contribute: Not smoking; Moderate alcohol consumption, and; having money.
In Australian men aged between 65 and 83, those who engaged in about 30 minutes of exercise five or so times per week were much healthier and less likely to be dead 11 years after the start of the study than those who were sedentary, even when the researchers adjusted for smoking habits, education, body mass index and other variables.
Offering hope and encouragement to the many adults who have somehow neglected to exercise for the past few decades, a new study suggests that becoming physically active in middle age, even if someone has been sedentary for years, substantially reduces the likelihood that he or she will become seriously ill or physically disabled in retirement.
The new study joins a growing body of research examining successful aging, a topic of considerable scientific interest, as the populations of the United States and Europe grow older, and so do many scientists. When the term is used in research, successful aging means more than simply remaining alive, although that, obviously, is the baseline requirement. Successful aging involves minimal debility past the age of 65 or so, with little or no serious chronic disease diagnoses, depression, cognitive decline or physical infirmities that would prevent someone from living independently.
Previous epidemiological studies have found that several, unsurprising factors contribute to successful aging. Not smoking is one, as is moderate alcohol consumption, and so, unfairly or not, is having money. People with greater economic resources tend to develop fewer health problems later in life than people who are not well-off.
But being physically active during adulthood is particularly important. In one large-scale study published last fall that looked at more than 12,000 Australian men aged between 65 and 83, those who engaged in about 30 minutes of exercise five or so times per week were much healthier and less likely to be dead 11 years after the start of the study than those who were sedentary, even when the researchers adjusted for smoking habits, education, body mass index and other variables.
Whether exercise habits need to have been established and maintained throughout adulthood, however, in order to affect aging has been less clear. If someone has slacked off on his or her exercise resolutions during young adulthood and early middle-age, in other words, is it too late to start exercising and still have a meaningful impact on health and longevity in later life?
To address that issue, researchers with the Physical Activity Research Group at University College London and other institutions turned recently to the large trove of data contained in the ongoing English Longitudinal Study of Aging, which has tracked the health habits of tens of thousands of British citizens for decades, checking in with participants multiple times and asking them how they currently eat, exercise, feel and generally live.
For the study, appearing in the February issue of the British Journal of Sports Medicine, scientists isolated responses from 3,454 healthy, disease-free British men and women aged between 55 and 73 who, upon joining the original study of aging, had provided clear details about their exercise habits, as well as their health, and who then had repeated that information after an additional eight years.
The researchers stratified the chosen respondents into those who were physically active or not at the study’s start, using the extremely generous definition of one hour per week of moderate or vigorous activity to qualify someone as active. Formal exercise was not required. An hour per week of “gardening, cleaning the car, walking at a moderate pace, or dancing” counted, said Mark Hamer, a researcher at University College London who led the study.
The scientists then re-sorted the respondents after the eight-year follow-up, marking them as having remained active, become active, remained inactive or become inactive as they moved into and through middle-age. They also quantified each respondent’s health throughout those years, based on diagnosed diabetes, heart disease, dementia or other serious conditions. And the scientists directly contacted their respondents, asking each to complete objective tests of memory and thinking, and a few to wear an activity monitor for a week, to determine whether self-reported levels of physical activity matched actual levels of physical activity. (They did.)
In the eight years between the study’s start and end, the data showed, those respondents who had been and remained physically active aged most successfully, with the lowest incidence of major chronic diseases, memory loss and physical disability. But those people who became active in middle-age after having been sedentary in prior years, about 9 percent of the total, aged almost as successfully. These late-in-life exercisers had about a seven-fold reduction in their risk of becoming ill or infirm after eight years compared with those who became or remained sedentary, even when the researchers took into account smoking, wealth and other factors.
Those results reaffirm both other science and common sense. Anoteworthy 2009 study of more than 2,000 middle-aged men, for instance, found that those who started to exercise after the age of 50 were far less likely to die during the next 35 years than those who were and remained sedentary. “The reduction in mortality associated with increased physical activity was similar to that associated with smoking cessation,” the researchers concluded.
But in this study, the volunteers did not merely live longer; they lived better than those who were not active, making the message inarguable for those of us in mid-life. “Build activity into your daily life,” Dr. Hamer said. Or, in concrete terms, if you don’t already, dance, wash your car and, if your talents allow (mine don’t), combine the two.
Five signs that Apple is creating a health product
Malay Gandhi
February 03, 2014
Last week, Apple announced record quarterly revenue and earnings and was subsequently rewarded with almost 10% of its stock value being wiped out. Analysts cited anemic growth for the tech giant, and apparent saturation in the high-end smartphone market. Not surprisingly, many investors are wondering whether the category invented by the iPhone was a once in a lifetime opportunity. In fact, smartphones represent an era of computing that has far exceeded the previous era of personal computers in both install base and usage. Apple seems less concerned, perhaps because their eyes are set on the next era of computing—wearables.
Over the past year, Apple has been quietly building up the resources necessary to release a health product of their own. If the past continues to repeat itself, the digital health landscape could see a huge shift as the standard setter works to create a product that consumers love and use. Culminating in a meeting late last year between senior Apple execs and the FDA, here are five signs that a potentially game-changing digital health product is on the horizon.
1. “The whole sensor field is going to explode.” -Apple CEO Tim Cook
Tim Cook has indicated that wearables are an area of intense interest for Apple, labeling it as a “key branch of the tree” for the post-PC world at D11 last year.
2. The M7 coprocessor.
Apple has already released dedicated hardware for tracking health. The M7 coprocessor is included in every iPhone 5s and has been designed specifically to monitor physical activity, using motion data from the phone’s embedded sensors. The chip has been engineered from the ground up to sip power, extending battery life while allowing for high resolution capture of activity data. Leading fitness apps including Moves, Nike+ Move and Fitbit’s MobileTrack feature take advantage of the new hardware.
Shipping this component in the high volume iPhone product category has allowed Apple to bring the M7 to scale much faster than if they had initially released it within a new product category. The company’s relentless focus on integrated hardware and software experience has allowed them to achieve unmatched performance, and battery life is likely to be one of the keys to winning in wearables.
Bonus: With its “secure enclave” in the A7 processor designed for managing fingerprint data, Apple has also proven it can manage biometric data that is intended to be kept highly secure.
3. They’re hiring medical device experts.
Ravi Narasimhan, a Stanford PhD with expertise in “biomedical algorithms, data analysis and wireless technologies” and former VP of R&D in Biosensor Technologies at Vital Connect joined Apple in December 2013 (LinkedIn).
Nancy Dougherty, who previously worked at digital health sensor startups Proteus and Sano Intelligence, was hired in December (LinkedIn).
Michael O’Reilly, the former CMO of Masimo, developers of a pulse oximeter for the iPhone, joined Apple in July (LinkedIn).
Dr. Todd Whitehurst, a self-proclaimed “medical device R&D professional” and former VP of Product Development of Senseonics, a developer of glucose sensors, joined Apple 8 months ago as a Director of Hardware Development (LinkedIn).
Ueyn Block who was formerly with C8 MediSensors developing “non-invasive measurement of substances in the human body” joined 10 months ago as a Technical Lead for Optical Sensing (LinkedIn).
Yuming Liu, who previously worked at O2MedTech and Accuvein, was hired as an Analog Engineer (LinkedIn).
Bob Mansfield, Apple’s longtime lead for hardware engineering, was lured out of retirement to develop unspecified “future products.” The New York Times reports that Mansfield has been exploring sensor technologies for health and is directly involved with the future smartwatch project.
4. Intellectual property.
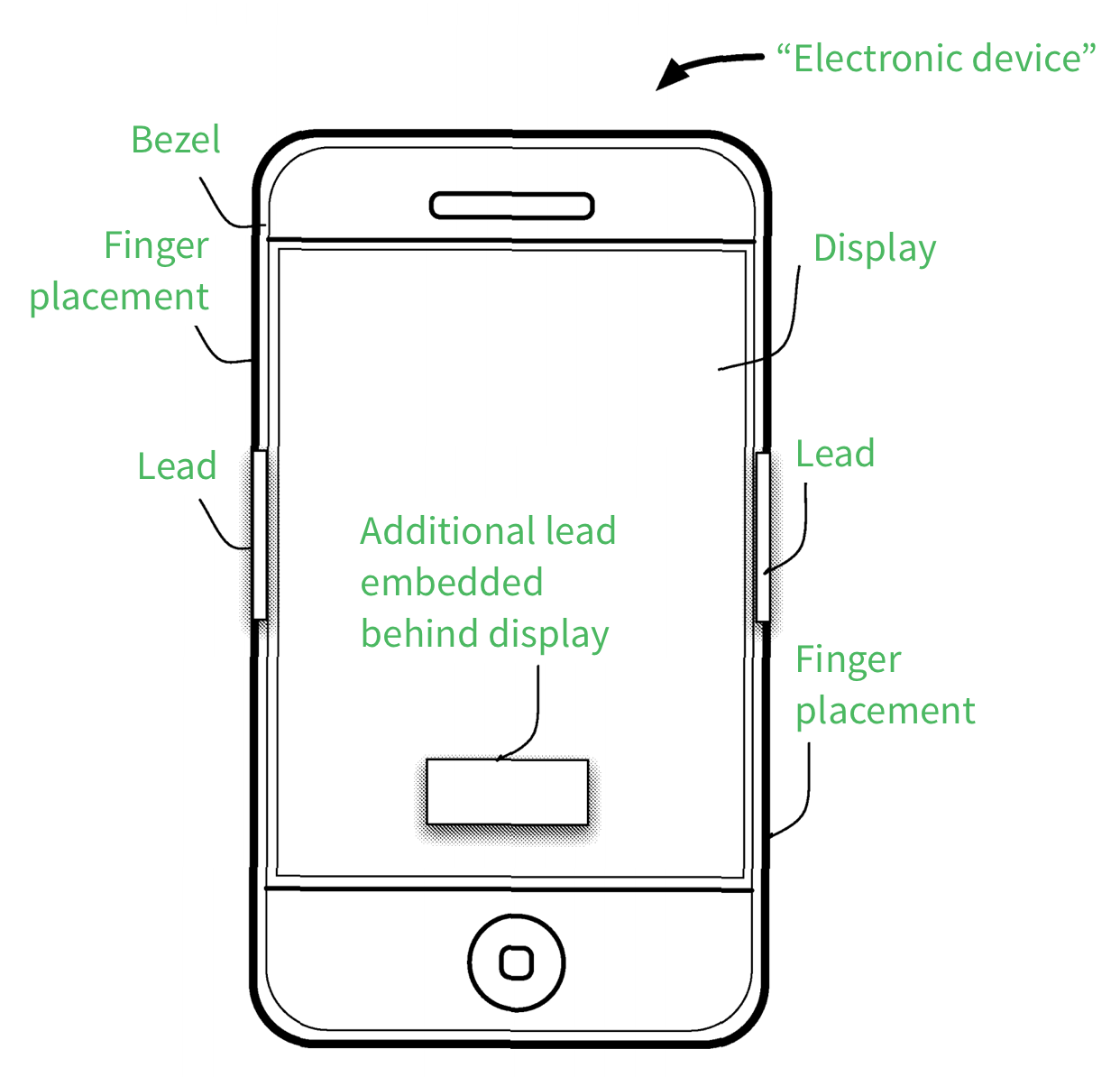
In 2009, Apple filed a patent for a “seamlessly embedded heart rate monitor” and was ultimatelyawarded the patent by the United States Patent and Trademark Office (USPTO) in late 2013. The patent covers the use of embedded sensors to measure a user’s heartbeat, heart rate, or other cardiac signals. The patent further covers locating the leads in accessories, such as headphones (or perhaps a wearable device).
Source: USPTO, annotations by Rock Health
Apple has also explored using personal area networks that would cover items such as the “event monitor device” (EMD) that would include an adhesive strip, a processor, a detector, and a communications port. The patent provides an example of monitoring an individual’s heart rate for events over a threshold (e.g., 180 beats per minute). While such a device sounds familiar to iRhytm’s Zio patch, the patent suggests Apple is looking more broadly into the development of an ecosystem of products that would be anchored by a single wearable platform device (likely wrist-worn), and augmented through various hardware sensors that could live in, on, or around the body and communicate with the primary device.
Source: USPTO, annotations by Rock Health
Most recently, Patently Apple has uncovered a patent application for a medical app that can monitor physiological data (e.g., arrhythmias), and either store it on a device like an iPhone and/or transmit the data to health facilities via a communication network. The patent was filed by Naeem Ansari, who was also behind a recent financial system patent that was ultimately assigned to Apple.
5. Check-in with the Food and Drug Administration (FDA).
Senior Apple executives met with FDA leadership, including the Director of the Agency’s Center for Devices and Radiological Health, which has oversight of medical devices, and Bakul Patel, the author of the FDA’s guidance on mobile medical applications. Patel’s guidance indicates that any mobile technologies which are intended for use in the diagnosis of a medical condition, or in the cure, mitigation or treatment of one will be regulated as medical devices.
Eric Horwitz leading the way on mining twitter feeds for signs of depression
He muses on looking at the impact of news on mood at a population level
Conway’s team is looking at some of the tough ethical questions involved, by “investigating public attitudes towards the ethics of using social media for public health monitoring,” he says. “This ethical component of the work is particularly important given the evolving role of social media in society and concerns regarding the activities of the NSA.”
With its 230 million regular users, Twitter has become such a broad stream of personal expression that researchers are beginning to use it as a tool to dig into public health problems. Believe it or not, a scientist out there might actually care about the sandwich you ate for lunch—even if most of your followers don’t.
“Our attitude is that Twitter is the largest observational study of human behavior we’ve ever known, and we’re working very hard to take advantage of it,” explains Tyler McCormick of the Center for Statistics and the Social Sciences at the University of Washington.
What if, for example, an artificial intelligence model could scan your Twitter feed and tell you if you’re at risk for depression? And what if you could receive notices from third parties, for instance, that warned you that you may want to seek help, just based on an automated scan of your tweets? Eric Horvitz, co-director of Microsoft Research Redmond has helped pioneer research on Twitter and depression. He says that could one day be a possibility.
“We wondered if we could actually build measures that might be able to detect if someone is severely depressed, just in publicly posted media. What are people telling the world in public spaces?” asks Horvitz. “You might imagine tools that could make people aware of a swing in mood, even before they can feel it themselves.”
Horvitz and a team of researchers helped develop a model that can scan tweets and predict depression in Twitter users, with an accuracy they claim to be 70%. Researchers say the system is still far from perfect. When the model scans your tweets, it misses some signals and doesn’t diagnose many people—about 30%—who really will get depression. And the system has a “false positive” issue, Horvitz said, causing it to incorrectly predict that healthy Twitter users will get depression in about 10% of cases.
The Microsoft team found 476 Twitter users, 171 of whom were seriously depressed. They went back into users’ Twitter histories as far as a year in advance of their depression diagnosis, examining their tweets for language, level of engagement, mentions of certain medications, and other factors, using computer models to sift through a total of 2.2 million tweets. By comparing depressed Twitter users’ feeds with the non-depressed user sample class, they came up with a method for predicting depression diagnoses before they happened. When they tested the model on a different set of Twitter users, it showed 70% accuracy in predicting depression before its onset.
Some tweets the scientists looked at in the depressed group pretty obviously indicate some level of emotional distress. For example, the study cited tweets like these from their depressed user group:
“Having a job again makes me happy. Less time to be depressed and eat all day while watching sad movies.”
“I want someone to hold me and be there for me when I’m sad.”
“‘Are you okay?’ Yes… I understand that I am upset and hopeless and nothing can help me… I’m okay… but I am not all right.”
Not all users’ feeds are so clear. Microsoft’s researchers looked at factors like the number of tweets users made per day, what time of day users tweeted, how often users interacted with each other, and what kind of language tweeters were using. For example, seemingly depressed tweeters were more likely to post messages late at night (between 9pm and 6am) compared with healthy tweeters, who were most active during the day and after work hours.
The team also noticed that certain isolated words in Twitter posts also were characteristic of depression. Words like anxiety, severe, appetite, suicidal, nausea, drowsiness, fatigue,nervousness, addictive, attacks, episodes, andsleep were used by depressed users, but more surprisingly, words like she, him, girl, game, men, home, fun, house, favorite, wants, tolerance, cope, amazing, love, care, songs, and movie could be indications of depression as well.
The volume of tweets mattered too, as did the percentage of exchanges—users who are depressed begin to tweet less, and tweet less at other people, indicating a possible loss of social connectedness, said Horvitz. Of course, just because a Twitter user makes a post that includes the word fatigue and house at 4am, that doesn’t mean they’re depressed. The Microsoft team’s classifier looked atusers’ feeds over long periods of time and incorporated many factors. A second Microsoft study that focused more on broader populations using slightly different methods achieved similar results, determining depression in tweets with around 70% accuracy.
One area of public health where this kind of research could come in handy is in measuring public reactions to events. Tracking public Twitter feeds after profound or traumatic events could help scientists understand how we’re affected by the news. “We really didn’t used to have many tools available traditionally for that kind of fine-grained analysis,” says said Horvitz. “Now there’s a new direction for doing the science.”
McCormick, of the University of Washington, said part of the research he and his team is now doing will involve improving earlier Twitter depression models, by weeding out false or misleading data and figuring out areas where depression-related data is being underreported. His team has also identified a group of first-year students at a number of colleges across the country based on their Twitter feeds—hashtags, posts relating to orientation—and is following them for “red flags” that could indicate emotional issues.
A study by University of California San Diego will also build on that research. Funded by the federal government’s National Institute of Health, UCSD’s Michael Conway is creating models that will eventually track depression in communities and figure out how to apply mental health resources better assess public health. “The ultimate goal of this work is to provide a cost-effective, real-time means of monitoring the prevalence of depression in the general population,” Conway said in an email.
In a post-Snowden era, privacy is a major concern facing any kind of mass-data collection. The Twitter users in the Microsoft study permitted Horvitz and his team to examine their tweets, but a possible future in which computer programs automatically sift through your tweets to make judgments on your health could understandably set off alarms with big data skeptics.
Conway’s team is looking at some of the tough ethical questions involved, by “investigating public attitudes towards the ethics of using social media for public health monitoring,” he says. “This ethical component of the work is particularly important given the evolving role of social media in society and concerns regarding the activities of the NSA.”
It may be some time before the research is developed enough for Twitter to warn individuals at risk for depression to seek help. Horvitz says part of what’s driven his research is the staggering number of suicides in the United States every year due to depression: 30,000. “If we can even save through interventions a few of those 30,000 people each year, it will make this research well worth it,” he said.





 Wearables are so hot right now. Apple
Wearables are so hot right now. Apple 

 Jon Feingersh/Getty Images
Jon Feingersh/Getty Images
 Malay Gandhi
Malay Gandhi