Health insurance companies are uniquely positioned to save the day in our ailing health system. Yes, you heard me correctly: health insurers.
Health insurers — or “payers” — are reviled nearly universally. Confused by “explanation of benefits” forms and denials of coverage and frustrated by rising deductibles, co-pays, and costs of care, consumers rank their experiences with health insurers below those with cable companies and internet service providers. Physicians and other care providers — who are constantly negotiating price of services and filling out piles of paperwork — don’t like payers much either.
All this makes insurers unlikely heroes. But we need someone to cut through the complexity of the current system, demand true value from providers, and create better options for consumers. Insurers increasingly look like the folks who can do the job and reinvent their business at the same time.
How? They can use their market power (they direct the bulk of health care dollars) and understanding of different consumer segments to create innovative products, services, and partnerships that address consumers’ needs. In the process, they can help move us all toward a low-cost, value-based health care system. Here are some specific ideas on what payers could do:
Act as true partners to value-based providers. Most payers today are piloting new economic models that pay providers not for the services they provide but for the value they create. Most, however, are neglecting a key opportunity: helping providers change their operating model. To succeed in value-based care, providers need data, analytics, smart clinical-care teams, and managerial support. Insurers are well-positioned to provide all this. They can also help providers become more efficient and assist them in navigating the tricky financial transition from fee-for-service to fee-for-value economics. Most important, insurers can help the very best provider organizations succeed by using them as the core of attractive, competitively priced insurance products.
Offer options for low-cost, convenient care. One area of waste in health care is the use of physician offices and hospital emergency departments to treat minor conditions such as sore throats, urinary infections, and allergies. Payers can make it easy for their members to get care 24/7 in more appropriate settings by partnering with retail, urgent care clinics, and telehealth providers. They can also offer the data connectivity needed to keep the consumer’s primary care provider in the loop. Oscar, the New York health insurance company launched last year, received fanfare in the press over its sleek offering, which includes unlimited phone and video calls with physicians and a “doctor on call” service that provides prescriptions by phone or e-visits. A number of retail pharmacy chains are also actively pursuing retail health and wellness clinics in stores to boost growth. Walmart has been piloting low-cost care clinics offering a $40 office visit that could dramatically reset the cost bar if scaled broadly.
Cover new wellness- and prevention-oriented treatments. Such options can serve as effective adjuncts to traditional benefits and encourage the trend toward more self-care. Aetna, for example, has offered mindfulness and yoga training to 6,000 of its employees. Its research shows that lower employee stress improved productivity by 69 minutes per week and gave an 11:1 return on investment. Similarly, articles in The New York Times, TIME, Scientific American, JAMA, and The Huffington Post cite growing evidence of the efficacy of meditation programs.
Explode the PPO model. Today the gold standard for health insurance is a preferred provider organization, a huge collection of doctors assembled to provide something for everyone but no special benefit to anyone. Insurers can do a better job for consumers and create real value by developing hassle-free mass customization. In this new model, consumers can choose from lifestyle-based curated options that offer trade-offs across risk level, health-savings options, primary-care models, alternative networks, network breadth, coaching and navigation programs, rewards programs, contract length, and incentive structures. Transparency tools and crowd-sourced reviews will spotlight value and multi-modal coordinated care delivery (think care teams that seamlessly work with telehealth providers, health coaches, and retail clinics) will help cut costs considerably. Consumers will be able to trade their own health engagement into benefit dollars and rewards that they can use seamlessly. While true à la carte insurance customization is not yet a reality, private exchange platforms are starting to provide a stepping stone to get there. For example, Maxwell Health, a new private exchange platform, presents a beautiful interface with lifestyle-focused packages that make product selection simple and tailored for you.
Sell convenience and personalized service. Most health care could hardly be less convenient. Now that consumers have unprecedented purchasing power (rise of public and private exchanges) and bear unprecedented costs (mounting high deductibles and premiums), they expect iPhone-like service. There is tremendous opportunity for payers to make the health care experience simpler and more supportive with online appointment scheduling, clear data and reviews, personalized suggestions, navigation apps with predictive decision support, reward programs, peer-to-peer support, and many other tools. Making the consumer experience better is smart for payers too. They can build stickier consumer relationships and generate new opportunities to address consumers’ growing health and lifestyle needs.
Power healthy behavior change. Some 50% of the determinants of health are driven by lifestyle and personal behaviors. Changing people’s behavior is a tall order but is necessary to improve health care. There are already examples of innovators that are succeeding, such as Omada Health with weight loss for pre-diabetics and Zipongo with healthy eating. We’ve only begun to deploy behavioral science, advanced wearable/monitoring technologies, and machine learning to understand the behaviors and motivations of different groups to predict and prevent acute events and connect people with the solutions that work best for them.
Serve as the bridge between new tools and consumers. In the first half of 2014,venture capital investment in digital health grew by 176%, spawning new consumer-centric companies with interesting approaches to consumer health. But there’s a chasm between these unscaled point solutions and the consumers who could use them. Payers can bridge the gap, using Amazon-style analytics and personalization to better understand consumer types and then connect them at the right place and time to the best-suited offerings. Better yet, payers don’t need to build the bridge themselves: A growing set of powerful consumer-engagement platforms (e.g., WellTok and Optum’s Rally) are moving along this path.
Payers have economic incentives to do everything I’ve described. The Affordable Care Act puts limits on the margins they can earn from their traditional business (Oliver Wyman estimates payer margins may shrink by a third), and an evolving marketplace means that they will face significantly more competition — from each other, health care providers, and new entrants that see an opportunity to capture growth in a $3 trillion market. The options I’ve described would let payers move into non-regulated markets and potentially generate revenue from discretionary consumer spending — a growing pot of money they have not accessed much.
Can they win consumers over? One advantage of being in an industry people don’t like is that there are many opportunities to pleasantly surprise the consumer. The good news is that the things that will make consumers happy — more convenience, customization, support for doctors, coordination of care — can all contribute to attractive new business opportunities while making the health care system more efficient, effective, humane, and sustainable.
Sukanya Soderland is a partner in Oliver Wyman’s Health and Life Sciences practice and a leader in the firm’s Health Innovation Center.
Which surgeon you get matters — a lot. But how do we know who the good ones are?
“You can think of surgery as not really that different than golf.” Peter Scardino is the chief of surgery at Memorial Sloan Kettering Cancer Center (MSK). He has performed more than 4,000 open radical prostatectomies. “Very good athletes and intelligent people can be wildly different in their ability to drive or chip or putt. I think the same thing’s true in the operating room.”
The difference is that golfers keep score. Andrew Vickers, a biostatistician at MSK, would hear cancer surgeons at the hospital having heated debates about, say, how often they took out a patient’s whole kidney versus just a part of it. “Wait a minute,” he remembers thinking. “Don’t you know this?”
“How come they didn’t know this already?”
In the summer of 2009, he and Scardino teamed up to begin work on a software project, called Amplio (from the Latin for “to improve”), to give surgeons detailed feedback about their performance. The program—still in its early stages but already starting to be shared with other hospitals — started with a simple premise: the only way a surgeon is going to get better is if he knows where he stands.
Vickers likes to put it this way. His brother-in-law is a bond salesman, and you can ask him, How’d you do last week?, and he’ll tell you not just his own numbers, but the numbers for his whole group.
Why should it be any different when lives are in the balance?
Andrew Vickers
The central technique of Amplio, using outcome data to determine which surgeons were more successful, and why, takes on a powerful taboo. Perhaps the longest-standing impediment to research into surgical outcomes — the reason that surgeons, unlike bond salesmen (or pilots or athletes), are so much in the dark about their own performance — are the surgeons themselves.
“Surgeons basically deeply believe that if I’m a well-trained surgeon, if I’ve gone through a good residency program, a fellowship program, and I’m board-certified, I can do an operation just as well as you can,” Scardino says. “And the difference between our results is really because I’m willing to take on the challenging patients.”
It is, maybe, a vestige of the old myth that anyone ordained to cut into healthy flesh is thereby made a minor god. It’s the belief that there are no differences in skill, and that even if there were differences, surgery is so complicated and multifaceted, and so much determined by the patient you happen to be operating on, that no one would ever be able to tell.
Vickers said to me that after several years of hearing this, he became so frustrated that he sat down with his ten-year-old daughter and conducted a little experiment. He searched YouTube for “radical prostatectomy” and found two clips, one from a highly respected surgeon and one from a surgeon who was rumored to be less skilled. He showed his daughter a 15second clip of each and asked, “Which one is better?”
“That one,” she replied right away.
When Vickers asked her why, “She looked at me, like, can’t you tell the difference? You can just see.”
Would you want to be cut by this surgeon?Or this one?
A remarkable paper published last year in the New England Journal of Medicine showed that maybe Vickers’s daughter was onto something.
In the study, run by John Birkmeyer, a surgeon who at the time was at the University of Michigan, bariatric surgeons were recruited from around the state of Michigan to submit videos of themselves doing a gastric bypass operation. The videos were sent to another pool of bariatric surgeons to be given a series of 1-to-5 rating on factors such as “respect for tissue,” “time and motion,” “economy of movement” and “flow of operation.”
The study’s key finding was that not only could you reliably determine a surgeon’s skill by watching them on video — skill was nowhere near as nebulous as had been assumed — but that those ratings were highly correlated with outcomes: “As compared with patients treated by surgeons with high skill ratings, patients treated by surgeons with low skill ratings were at least twice as likely to die, have complications, undergo reoperation, and be readmitted after hospital discharge,” Birkmeyer and his colleagues wrote in the paper.
You can actually watch a couple of these videos yourself [see above]. Along with the overall study results, Birkmeyer published two short clips: one from a highly rated surgeon and one from a low-rated surgeon. The difference is astonishing.
You see the higher-rated surgeon first. It’s what you always imagined surgery might look like. The robot hands move with purpose — quick, deliberate strokes. There’s no wasted motion. When they grip or sew or staple tissue, it’s with a mix of command and gentle respect. The surgeon seems to know exactly what to do next. The way they’ve set things up makes it feel roomy in there, and tidy.
Watching the lower-rated surgeon, by contrast, is like watching the hidden camera footage of a nanny hitting your kid: it looks like abuse. The surgeon’s view is all muddled, they’re groping aimlessly at flesh, desperate to find purchase somewhere, or an orientation, as if their instruments are being thrashed around in the undertow of the patient’s guts. It’s like watching middle schoolers play soccer: the game seems to make no sense, to have no plot or direction or purpose or boundary. It’s not, in other words, like, “This one’s hands are a bit shaky,” it’s more like, “Does this one have any clue what they’re doing?”
It’s funny: in other disciplines we reserve the word “surgical” for feats that took a special poise, a kind of deftness under pressure. But the thing we maybe forget is that not all surgery is worthy of the name.
Vickers is best known for showing exactly how much variety there is, plotting, in 2007, the so-called “learning curve” for surgery: a graph that tracks, on one axis, the number of cases a surgeon has under his belt, and on the other, his recurrence rates (the rate at which his patients’ cancer comes back).
As surgeons get more experience, their patients do better. This “learning curve” shows patients’ 5 year cancer-free rates rise with procedure volume.
He showed that in incidents of prostate cancer that haven’t spread beyond the prostate — so-called ‘organ-confined’ cases — the recurrence rates for a novice surgeon were 10 to 15%. For an experienced surgeon, they were less than 1%. With recurrence rates so low for the most experienced surgeons, Vickers was able to conclude that in organ-confined cancer cases, the onlyreason a patient would recur is “because the surgeon screwed up.”
There’s a large literature, going back to a famous paper in 1979, finding that hospitals with higher volumes of a given surgical procedure have better outcomes. In the ’79 study it was reported that for some kinds of surgery, hospitals that saw 200 or more cases per year had death rates that were 25% to 41% lower than hospitals with lower volumes. If every case were treated at a high-volume hospital, you would avoid more than a third of the deaths associated with the procedure.
But what wasn’t clear was why higher volumes led to better outcomes. And for decades, researchers penned more than 300 studies restating the same basic relationship, without getting any closer to explaining it. Did low-volume hospitals end up with the riskiest patients? Did high-volume hospitals have fancier equipment? Or better operating room teams? A better overall staff? An editorial as late as 2003 summarized the literature with the title, “The Volume–Outcome Conundrum.”
A 2003 paper by Birkmeyer, “Surgeon volume and operative mortality in the United States,” was the first to offer definitive evidence that the biggest factor determining the outcome of many surgical procedures — the hidden element that explained most of the variation among hospitals — was the procedure volume not of the hospital, but of the individual surgeons.
“In general I don’t think anyone was surprised that there was a learning curve,” Vickers says. “I think they were surprised at what a big difference it made.” Surprised, maybe, but not moved to action. “You may think that everyone would drop what they were doing,” he says, “and try and work out what it is that some surgeons are doing that the other ones aren’t… But things move a lot more slowly than that.”
Tired of waiting, Vickers started sharing some initial ideas with Scardino about the program that would become Amplio. It would give surgeons detailed feedback about their performance. It would show you not just your own results, but the results for everyone in your service. If another surgeon was doing particularly well, you could find out what accounted for the difference; if your own numbers dropped, you’d know to make an adjustment. Vickers explains that they wanted to “stop doing studies showing surgeons had different outcomes.”
“Let’s do something about it,” he told Scardino.
Dr. Scardino
The first time I heard about Amplio was on the third floor of the Chrysler Building, in a room they called the Innovation Lab — the very room you’d point to if the Martians ever asked you what a 125-year old bureaucracy looks like. As I arrived, the receptionist was trying to straighten up a small mess of papers, post-its, cookies, and coffee stirrers. “The last crowd had a wild time,” she said. Every surface in the room was gray or off-white, the color of questionable eggs. It smelled like hospital-grade hand soap.
The people who filed in, though, and introduced themselves to each other (this was a summit of sorts, a “Collaboration Meeting” where different research groups from around MSK shared their works in progress) looked straight out of a well-funded biotech startup. There was a Fulbright scholar; a double-major in biology and philosophy; a couple of epidemiologists; a mathematician; a master’s in biostats and predictive analytics. There were Harvards, Cals, and Columbias, bright-eyed and sharply dressed.
Vickers was one of the speakers. He’s in his forties but he looks younger, less like an academic than a seasoned ski instructor, a consequence, maybe, of the long wavy hair, or the well-worn smile lines around his eyes, or this expression he has that’s like a mix of relaxed and impish. He leans back when he talks, and he talks well, and you get the sense that he knows he talks well. He’s British, from north London, educated first at Cambridge and then, for his PhD in clinical medicine, at Oxford.
The first big task with Amplio, he said, was to get the data. In order for surgeons to improve, they have to know how well they’re doing. In order to know how well they’re doing, they have to know how well their patients are doing. And this turns out to be trickier than you’d think. You need an apparatus that not only keeps meticulous records, but keeps them consistently, and throughout the entire life cycle of the patient.
That is, you need data on the patient before the operation: How old are they? What medications are they allergic to? Have they been in surgery before? You need data on what happened during the operation: where’d you make your incisions? how much blood was lost? how long did it take?
And finally, you need data on what happened to the patient after the operation — in some cases years after. In many hospitals, followup is sporadic at best. So before the Amplio team did anything fancy, they had to devise a better way to collect data from patients. They had to do stuff like find out whether it was better to give the patient a survey before or after a consultation with their surgeon? And what kinds of questions worked best? And who were they supposed to hand the iPad to when they were done?
Only when all these questions were answered, and a stream of regular data was being saved for every procedure, could Amplio start presenting something for surgeons to use.
A screen in Amplio shows how a surgeon’s patients are doing against their colleagues’
After years of setup, Amplio now is in a state where it can begin to affect procedures. The way it works is that a surgeon logs into a screen that shows where they stand on a series of plots. On each plot there’s a single red dot sitting amid some blue dots. The red dot shows your outcomes; the blue dots show the outcomes for each of the other surgeons in your group.
You can slice and dice different things you’re interested in to make different kinds of plots. One plot might show the average amount of blood lost during the operation against the average length of the hospital stay after it. Another plot might show a prostate patient’s recurrence rates against his continence or erectile function.
There’s something powerful about having outcomes graphed so starkly. Vickers says that there was a surgeon who saw that they were so far into the wrong corner of that plot — patients weren’t recovering well, and the cancer was coming back — that they decided to stop doing the procedure. The men spared poor outcomes by this decision will never know that Amplio saved them.
It’s like an analytics dashboard, or a leaderboard, or a report card, or… well, it’s like a lot of things that have existed in a lot of other fields for a long time. And it kind of makes you wonder, why has it taken so long for a tool like this to come to surgeons?
The answer is that Amplio has cleverly avoided the pitfalls of some previous efforts. For instance, in 1989, New York state began publicly reporting the mortality rates of cardiovascular surgeons. Because the data was “risk-adjusted”—an unfavorable outcome would be considered less bad, or not counted at all, if the patient was at risk to begin with — surgeons started pretending their patients were a lot worse off than they were. In some cases, they avoided patients who looked like goners. “The sickest patients weren’t being treated,” Vickers says. One investigation into why mortality in New York had dropped for a certain procedure, the coronary artery bypass graft, concluded that it was just because New York hospitals were sending the highest-risk patients to Ohio.
Vickers wanted to resist such gaming. But the answer is not to quit adjusting for patient risk. After all, if a given report says that your patients have 60% fewer complications than mine, does that mean that you’re a 60% better surgeon? It depends on the patients we see. It turns out that maybe the best way to prevent gaming is just to keep the results confidential. That sounds counter to a patient’s interests, but it’s been shown that patients actually make little use of objective outcomes data when it’s available, that in fact they’re much more likely to choose a surgeon or hospital based on reputation or raw proximity.
With Amplio, since patients, and the hospital, and even your boss are blinded from knowing whose results belong to whom, there’s no incentive to fudge risk factors or insist that a risk factor’s weight be changed, unless you think it’s actually good for the analysis.
That’s why Amplio’s interface for slicing and dicing the data in multiple ways matters, too. Feedback systems in the past that have given surgeons a single-dimensional report — say, they only track recurrence rates — have failed by creating a perverse incentive to optimize along just that one dimension, at the expense of all the others. Another reminder that feedback is, like surgery itself, fraught with complication: if you do it wrong, it can be worse than useless.
Every member of the Amplio team I spoke to stressed this point over and over again, that the system had been painstakingly built from the “bottom up” — tuned via detailed conversations with surgeons (“Are you accounting for BMI? What if we change the definition of blood loss?”) — so that the numbers it reported would be accurate, and risk-adjusted, and multidimensional, and credible. Because only then would they be actionable.
Karim Touijer, a surgeon at MSK who has used Amplio, explains the system’s chief benefit is the fact that you can vividly see how you’re doing, and that someone else is doing better. “When you set a standard,” he says, “the majority of people will improve or meet that standard. You tend to shrink the outliers. If I’m an outlier, if my performance leaves something to be desired, then I can go to my colleagues and say what is it that you’re doing to get these results?” Touijer sees this as the gradual standardization of surgery: you find the best performers, figure out what makes them good, and spread the word. He said that already within his group, because the conversations are more tied to outcomes, they’re talking about technique in a more objective way.
In fact, he says, as a result of Amplio he and his team have devised the first randomized clinical trial that is solely dedicated to surgical maneuvers.
Touijer specializes in the radical prostatectomy, considered one of the most complex and delicate operations in all of surgical practice. The procedure — in which a patient’s cancerous prostate is entirely removed — is highly sensitive to an individual surgeon’s skill. The reason is that the cancer ends up being very close to the nerves that control sexual and urinary function. It’s an operation unlike, say, kidney cancer, where you can easily go widely around the cancer. If you operate too far around the prostate, you could easily damage the rectum, the bladder, the nerves responsible for erection, or the sphincter responsible for urinary control. “It turns out that radical prostatectomy is very, very intimately influenced by surgical technique,” Touijer says. “One millimeter on one side or less than a millimeter on the other can change the outcome.”
Option B in the first A/B test for surgery: “A second bite is taken deeply into the fascia of the lateral pelvic fascia”
There’s a moment during the procedure where the surgeon has to decide whether to make a particular stitch. Some surgeons do it, some don’t; we don’t yet know which way is better. In the randomized trial, if the surgeon doesn’t have a compelling reason to pick one of the two alternatives, he lets the computer decide randomly for him. With enough patients, it should be possible to isolate the effect of that one decision, and to find out whether the extra stitch leads to better outcomes. The beauty is, since the outcomes data was already being tracked, and the patients were already going to have the surgery, the trial costs almost nothing.
If you’ve worked on the web, this model of rapid, cheap experimentation probably sounds familiar: what Touijer is describing is the first A/B test for surgery. As it turns out this particular test didn’t yield significant results. But several other tests are in the works, and some may improve some specific surgical techniques—improving the odds for all patients.
In Better, Atul Gawande argues that when we think of improving medicine, we always imagine making new advances, discovering the gene responsible for a disease, and so on — and forget that we can simply take what we already know how to do, and figure out how to do it better. In a word, iterate.
“But to do that,” Scardino says, “we have to measure it, we have to know what the results are.”
Scardino describes how when laparascopy was first becoming an option for radical prostatectomy, there was a lot of hype. “The company and many doctors who were doing it immediately claimed that it was safer, had better results, was more likely to cure the cancer and less likely to have permanent urinary or sexual problems.” But, he says, the data to support it were weak, and biased. “We could see in Amplio early on that as people started doing robotic surgery, the results were clearly worse.” It took time for them to hit par with the traditional open procedure; it took time for them to get better.
After a pilot among prostate surgeons, Amplio spread quickly to other services within MSK, including for kidney cancer, bladder cancer and colorectal cancer. Vickers’s team has been working with other hospitals — including Columbia in New York, the Barbara Ann Karmanos Cancer Institute in Michigan, and the MD Anderson Cancer Center in Texas — to slowly begin integrating with their systems. But it’s still early days: even within their own hospital, surgeons were wary of Amplio. It took many conversations, and assurances, to convince them that the data were being collected for their benefit — not to “name and shame” bad performers.
We know what happens when performance feedback goes awry — similar efforts to “grade” American schoolteachers, for instance, have perhaps generated more controversy than results. To do performance feedback well requires patience, and tact, and an earnest imperative to improve everyone’s results, not just to find the negative outliers. But Vickers believes that enough surgeons have signed on that the taboo has been broken at MSK. And results are bound to flow from that.
It’s all about trust. Remember the Birkmeyer study that compared surgeons using videos? It was only possible because Birkmeyer had built up relationships by way of a previous outcomes experiment in Michigan that meticulously protected data. “That’s a question that we get really frequently,” Birkmeyer told me when we spoke about the paper. “How on earth did we ever pull that study off?” The key, he says, is that years of research with these surgeons had slowly built goodwill. When it came time to make a big ask, “the surgeons were at a place where they could trust that we weren’t gonna screw them.”
Amplio will no doubt have to be able to say the same thing, if it’s to spread beyond the country’s best research cancer centers into the average regional hospital.
In 1914, a surgeon at Mass General got so fed up with the administration, and their refusal to measure outcomes, that he created his own private hospital, “the End Result Hospital,” where detailed records were to be kept of every patient’s “end results.” He published the first five years of his hospital’s cases in a book that became one of the founding documents of evidence-based medicine.
“The Idea is so simple as to seem childlike,” he wrote, “but we find it ignored in all Charitable Hospitals, and very largely in Private Hospitals. It is simply to follow the natural series of questions which any one asks in an individual case: What was the matter? Did they find it out beforehand? Did the patient get entirely well? If not — why not? Was it the fault of the surgeon, the disease, or the patient? What can we do to prevent similar failures in the future?”
It might finally be time for that simple, “childlike” concept to reach fruition. It’s like Vickers said to me one night in early November, as we were discussing Amplio, “Having been in health research for twenty years, there’s always that great quote of Martin Luther King: The arc of history is long, but it bends towards justice.”
WHEN we are patients, we want our doctors to make recommendations that are in our best interests as individuals. As physicians, we strive to do the same for our patients.
But financial forces largely hidden from the public are beginning to corrupt care and undermine the bond of trust between doctors and patients. Insurers, hospital networks and regulatory groups have put in place both rewards and punishments that can powerfully influence your doctor’s decisions.
Contracts for medical care that incorporate “pay for performance” direct physicians to meet strict metrics for testing and treatment. These metrics are population-based and generic, and do not take into account the individual characteristics and preferences of the patient or differing expert opinions on optimal practice.
For example, doctors are rewarded for keeping their patients’ cholesterol and blood pressure below certain target levels. For some patients, this is good medicine, but for others the benefits may not outweigh the risks. Treatment with drugs such as statins can cause significant side effects, including muscle pain and increased risk of diabetes. Blood-pressure therapy to meet an imposed target may lead to increased falls and fractures in older patients.
Physicians who meet their designated targets are not only rewarded with a bonus from the insurer but are also given high ratings on insurer websites. Physicians who deviate from such metrics are financially penalized through lower payments and are publicly shamed, listed on insurer websites in a lower tier. Further, their patients may be required to pay higher co-payments.
These measures are clearly designed to coerce physicians to comply with the metrics. Thus doctors may feel pressured to withhold treatment that they feel is required or feel forced to recommend treatment whose risks may outweigh benefits.
It is not just treatment targets but also the particular medications to be used that are now often dictated by insurers. Commonly this is done by assigning a larger co-payment to certain drugs, a negative incentive for patients to choose higher-cost medications. But now some insurers are offering a positive financial incentive directly to physicians to use specific medications. For example, WellPoint, one of the largest private payers for health care, recently outlined designated treatment pathways for cancer and announced that it would pay physicians an incentive of $350 per month per patient treated on the designated pathway.
This has raised concern in the oncology community because there is considerable debate among experts about what is optimal. Dr. Margaret A. Tempero of the National Comprehensive Cancer Network observed that every day oncologists saw patients for whom deviation from treatment guidelines made sense: “Will oncologists be reluctant to make these decisions because of an adverse effects on payments?” Further, some health care networks limit the ability of a patient to get a second opinion by going outside the network. The patient is financially penalized with large co-payments or no coverage at all. Additionally, the physician who refers the patient out of network risks censure from the network administration.
When a patient asks “Is this treatment right for me?” the doctor faces a potential moral dilemma. How should he answer if the response is to his personal detriment? Some health policy experts suggest that there is no moral dilemma. They argue that it is obsolete for the doctor to approach each patient strictly as an individual; medical decisions should be made on the basis of what is best for the population as a whole.
We fear this approach can dangerously lead to “moral licensing” — the physician is able to rationalize forcing or withholding treatment, regardless of clinical judgment or patient preference, as acceptable for the good of the population.
Medicine has been appropriately criticized for its past paternalism, where doctors imposed their views on the patient. In recent years, however, the balance of power has shifted away from the physician to the patient, in large part because of access to clinical information on the web.
In truth, the power belongs to the insurers and regulators that control payment. There is now a new paternalism, largely invisible to the public, diminishing the autonomy of both doctor and patient.
In 2010, Congress passed the Physician Payments Sunshine Act to address potential conflicts of interest by making physician financial ties to pharmaceutical and device companies public on a federal website. We propose a similar public website to reveal the hidden coercive forces that may specify treatments and limit choices through pressures on the doctor.
Medical care is not just another marketplace commodity. Physicians should never have an incentive to override the best interests of their patients.
Patients arm themselves with information about product safety and efficacy gleaned from websites and online communities such as PatientsLikeMe, pore over cost and quality indicators from healthcare start-ups such as Castlight Health or HealthGrades, and comparison shop using information synthesized by their insurance providers.
Pharmaceutical and medical-device companies have been slow to adopt digitization. Here are five reasons they should get moving.
November 2014| bySastry Chilukuri, Rena Rosenberg, and Steve Van Kuiken
The US healthcare industry is undergoing a major transformation as healthcare reform encourages consumers to play a far more active decision-making role. Yet despite this traditionally business-to-business industry moving quickly to a business-to-consumer model, companies have been slow to join the digital movement. Unlike successful B2C companies in other industries—which offer mobile solutions, provide personalized product recommendations, and empower customer-service agents with a 360-degree view of the customer—most healthcare providers and payors are lagging, as are pharmaceutical companies and medical-device manufacturers. That’s problematic when customers are increasingly expecting a better, more personalized experience from companies taking advantage of the host of digital tools and analytics at their disposal.
Healthcare is not immune to this reality. The sudden increase in the individual market1through the creation of exchanges and growth in Medicare Advantage2 has forced US payors to adopt some of these digital tools, while the growing cost burden for healthcare absorbed by consumers inspires many would-be patients to jump on the web or social networks to conduct research. So why, with a few exceptions, are pharmaceutical and device companies taking a “wait and watch” approach? Government agencies, payors, disease advocates, and disrupters are launching digital solutions that threaten product sales and take advantage of the opportunity to respond to patient needs. This role should be a natural extension for pharmaceutical and medical-device companies, and we have identified five compelling reasons they must get moving before it is too late.
1. Patient behavior is changing
As with many other industries, consumers in the healthcare sector are becoming more informed, empowered, and demanding. The vast majority of connected patients are using an array of digital tools to take control of their health and the healthcare services they access and buy: more than 70 percent of patients who are online in the United States use the Internet to find healthcare information, and more than 40 percent of people who diagnosed their condition through online research had it confirmed by a physician.3Patients arm themselves with information about product safety and efficacy gleaned from websites and online communities such as PatientsLikeMe, pore over cost and quality indicators from healthcare start-ups such as Castlight Health or HealthGrades, and comparison shop using information synthesized by their insurance providers.
The more that healthcare data becomes digitally accessible, the more patients will use it to weigh—and potentially reject—expensive healthcare treatments. This is particularly true in the United States, where patients pay a greater percentage of the cost of their drug therapies (25 percent is not unusual) than they do for other healthcare expenses such as inpatient services. Not surprisingly, these consumers are demanding more information so they can apply the same cost-benefit analysis and research techniques they use to purchase cars or phones when they purchase healthcare; they are also making more informed, rational choices about where they put their money. Data and information about insurance plans, pharmaceutical products, and manufacturers are discussed in a variety of virtual forums. If companies do not join the digital dialogue and influence the conversation, they will lose an opportunity to shape it, and they may be put on the defensive trying to refute the statements made by those that do take part.
2. Government agencies are moving surprisingly quickly
As patient and consumer demand for information grows, the government is beginning to supply healthcare data either directly, through the release of information, or indirectly, by providing incentives for collection and aggregation of relevant clinical data. A recent McKinsey Global Institute report4 found that healthcare is one of seven sectors that could generate billions of dollars of value per year as companies use open data—machine-readable information made available to others, often free of charge—to develop new products and improve the efficiency and effectiveness of operations.
Government health agencies, from national health services in Asia and Europe to government organizations in the United States, are already harnessing the power of big data to figure out what’s working and what isn’t and encouraging others to do the same. The Health Data Initiative launched in 2010 by the US Department of Health & Human Services (HHS) was one of the first and is still among the most prominent examples. In June 2011, former HHS chief technology officer Todd Park described an ambition to make HHS the “NOAA of health data.”5 It appears that his vision is becoming reality, as HHS reported that more than 1,000 data sets were available on healthdata.gov at the end of 2013,6 and the agency’s catalog continues to expand.
The hope is that greater “data liquidity” will both enable more collaborative research among academics and inspire healthcare innovation. Greater access to data is already driving changes in care protocols, allowing the benchmarking of physicians, aiding the identification of clinical best practices, informing the adjustment of benefits and reimbursement structures, and resulting in actual behavioral change. At the federal level in the United States, for example, the recent release by the Centers for Medicare & Medicaid Services of Medicare reimbursements to providers put some physicians on the defensive to explain billing perceived as excessive, and the organization also proposed rescinding the prohibition against releasing prescriber, pharmacy, and plan identifiers related to Medicare Part D payments.
In another example, the new openFDA application-programming-interface initiative for drug-adverse events allows researchers to synthesize, interrogate, and generate insights from a decade (2004–13) of adverse-event reports—an effort that is almost certain to stir conversation. And at the US state level, Arkansas and Tennessee are examining treatment protocols and zeroing in on the relatively small number of care episodes that comprise the majority of medical costs. The states’ shared goal is cutting waste and revising reimbursement policies to encourage high-quality and efficient care.
These efforts mean that providers and manufacturers of drugs and devices only control a small fraction of the data relevant to their work or products. If healthcare follows the path of other consumer-oriented sectors that compete on data analytics, such as high tech and retailing, winners and losers will be determined in part by who makes the best use of the data available and the strongest case for change. Government agencies across the globe are leading the way, and entrepreneurs are taking advantage of government’s interest in facilitating data exchange. However, pharmaceutical and medical-device companies are on the sidelines, leaving others to dictate how information related to their products is used.
3. Trial data is necessary but no longer sufficient
Pharmaceutical companies have used data generated from long-running randomized controlled trials as the gold standard to demonstrate the efficacy and safety of products and gain regulatory approval or formulary listings. Yet many of their customers—payors, increasingly providers, and even patients—are looking for real-world evidence. Both access to and quality of real-world data are increasing exponentially, spanning everything from patient electronic health records to social platforms, healthcare claims, demographic trends, and genomic insights.
The difference in emphasis by certain stakeholders creates pressure on pharmaceutical companies to respond. As data integration and analyses take precedence over data ownership or sponsorship, competitive advantage will rest with those organizations that innovatively use multiple data sources to uncover true insights. Meeting long-standing requirements regarding clinical-trial data continues to be necessary for approval, but it is no longer enough for other stakeholders when more and more targeted and timely data are available. Consider this: Thomson Reuters found that the number of observational research studies tripled from roughly 80,000 between 1990 to 2000 to more than 263,000 in the following decade from 2001 through 2011.7
There is a concerted effort to facilitate collaboration by making more real-world data available at a fairly low cost. Initiatives such as PCORnet, a distributed research network, were launched to advance researchers’ ability to conduct comparative-effectiveness and clinical-outcomes research more efficiently. Aggregating data across “networks of networks” dramatically reduces the cost of observational studies and more quickly generates insights about patient care. Innovative methods enable randomization using real-world data to improve the quality of findings.
Pharmaceutical companies can’t discount observational data because such data already affect product pricing and reimbursement levels. European markets are using real-world evidence to limit reimbursements on new drugs to the competitor’s level until real-world evidence is provided to demonstrate that the new therapy is better. The International Society for Pharmacoeconomics and Outcomes Research reported in 2007 that countries were using reference pricing for new treatments assessed to add little incremental medical value, and real-world data was part of that effectiveness assessment.8 In short, pharmaceutical companies need a data strategy that reflects the shift in how data are shared and analyzed, as well as a plan to manage all types of data that affect product sales, pricing, and reimbursement.
4. Care is evolving
Healthcare is moving from a focus on addressing point-in-time issues toward coordinated, continuous health management. The need to provide ongoing management of chronic diseases and to predict and prevent severe episodes and events offers new opportunities and places new communication demands on every member of the healthcare team, including pharmaceutical companies. Sensor technology, such as that produced by Proteus Digital Health, allows continuous collection of physiological data (for example, electroencephalograph, electrocardiogram, movement, heart rate, and glucose levels), which could vastly improve disease management by providing real-time status reports that can alert providers to impending patient problems. When scaled broadly, these innovations also may reduce the need for many courses of treatment. Pharmaceutical companies need to be at the forefront of developing “beyond the pill” services that deliver value to patients and evolve from a mind-set that measures success based largely on the number of prescriptions written.
Some innovators already are combining technology-enabled monitoring and insight to deliver new solutions to patients. Propeller Health inserted GPS technology in inhalers to identify environmental triggers that caused asthma sufferers to use their device, thus allowing consumers to head off severe attacks. Similarly, a pharmaceutical company that made a pain medication equipped patients with Jawbone devices to continuously capture patient mobility. This showed that patients experienced greater relief that allowed them to increase their movement, even if they did not report lower pain scores. The evidence was used to convince payors to relist the pain medication on formularies.
Not all wraparound services rely on new technology. Telemedicine outreach and coaching efforts by nurses at one of the largest government hospital systems in the United States dramatically reduced the risk of complications from conditions such as diabetes.
Whether low or high tech, patient services aimed at preventing acute episodes or supporting compliance deliver significant benefits to patients. Pharmaceutical companies that remain fixated solely on prescription volume, rather than on sustaining relationships between a brand and patients, risk ceding the role of trusted provider to others. For industry participants to thrive in the digital era, they must build a broader menu of service offerings instead of merely using technology solutions to increase prescriptions.
5. Competition is faster and fiercer
Technology cycles are getting shorter and the cost of experimentation cheaper. The run-up to the passage of the Health Information Technology for Economic and Clinical Health Act in 2009 and Affordable Care Act in 2010 saw significant investment in companies developing systems, solutions, or applications to support electronic health records. From 2010 to the end of 2013, seed and Series A–stage healthcare investments continued to grow, multiplying fivefold in the United States in that time. In the first half of 2014, investors spent $2.3 billion, with more than 140 digital companies each raising more than $2 million,9 as the investment focus shifted from providers of electronic-health-records solutions to developers of consumer-oriented applications, makers of wearable health technology, and health data and analytics. There are thousands of healthcare-related apps available from the US Apple App Store, but only a fraction are patient facing with genuine health content, according to a new study from the IMS Institute for Healthcare Informatics. The recent announcement of the Apple Watch and the company’s release of its HealthKit developer tool are likely to increase the variety of functions and number of health-related apps that are available.
Google Glass is the most high-profile wearable being tested for numerous healthcare applications—for example, surgeons are using it to facilitate and record operations, office physicians are reducing interruptions in patient engagement by retrieving and sending information to electronic medical records through the device, and emergency-medicine physicians are getting specialist consults by transmitting video or images taken by Glass.10 Beyond Google, Intel acquired BASIS Science, MC10 raised a $41.9 million investment, and Proteus raised $183.4 million to develop its line of sensor-based products. Services or applications that facilitate consumer communication with doctors such as Doctor on Demand and HealthTap+ also secured financing.
These new entrants to the healthcare sector have different ways of thinking about solving healthcare problems and using proven agile iterative techniques to bring products to market rapidly and in iterations as improvements are made. Pharmaceutical companies need to recognize the value and impact of these disrupters and learn from them.
Digitally enabled healthcare is here, and most pharmaceutical companies aren’t ready. Despite access to unprecedented data and technologies that can be used to drive better health outcomes by influencing customer behavior, few are truly exploring digital-engagement models. The opportunity to learn more about consumers and develop better, more targeted products and services far outweighs the threat digitization presents companies—for now. Unless incumbent pharmaceutical companies move quickly, innovative competitors may grab a greater share of benefits and stronger customer loyalty.
About the authors
Sastry Chilukuri and Rena Rosenberg are principals in McKinsey’s New Jersey office, where Steve Van Kuiken is a director.
The authors wish to thank Elizabeth Doshi for her contribution to this article.
Sensible stuff. Possibly the most sensible stuff I’ve seen on this. Good for them…
How the world could better fight obesity
November 2014| byRichard Dobbs, Corinne Sawers, Fraser Thompson, James Manyika, Jonathan Woetzel, Peter Child, Sorcha McKenna, and Angela Spatharou
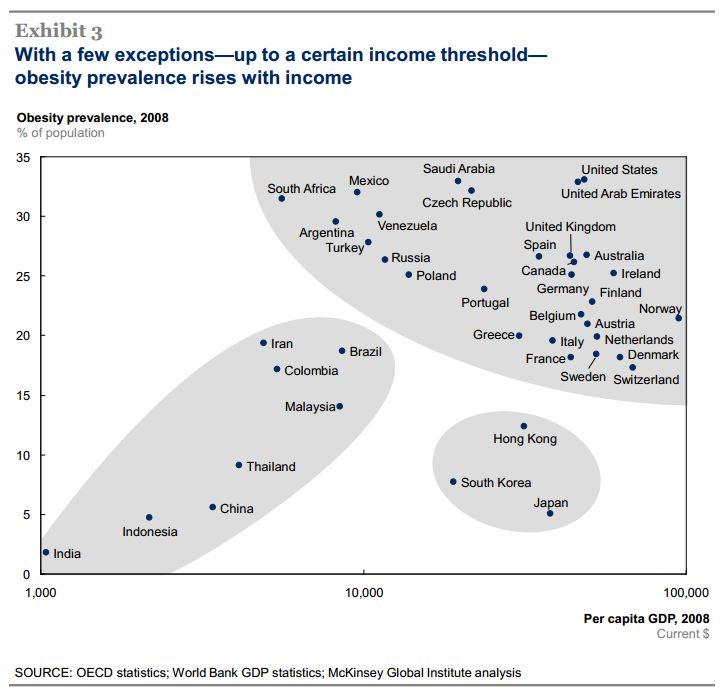
Obesity is a critical global issue that requires a comprehensive, international intervention strategy. More than 2.1 billion people—nearly 30 percent of the global population—are overweight or obese.1 That’s almost two and a half times the number of adults and children who are undernourished. Obesity is responsible for about 5 percent of all deaths a year worldwide, and its global economic impact amounts to roughly $2 trillion annually, or 2.8 percent of global GDP—nearly equivalent to the global impact of smoking or of armed violence, war, and terrorism.
MGI’s Richard Dobbs and Corinne Sawers discuss how a holistic strategy, using a number of interventions, could reverse rising rates of obesity around the world.
And the problem—which is preventable—is rapidly getting worse. If the prevalence of obesity continues on its current trajectory, almost half of the world’s adult population will be overweight or obese by 2030.
Much of the global debate on this issue has become polarized and sometimes deeply antagonistic. Obesity is a complex, systemic issue with no single or simple solution. The global discord surrounding how to move forward underscores the need for integrated assessments of potential solutions. Lack of progress on these fronts is obstructing efforts to address rising rates of obesity.
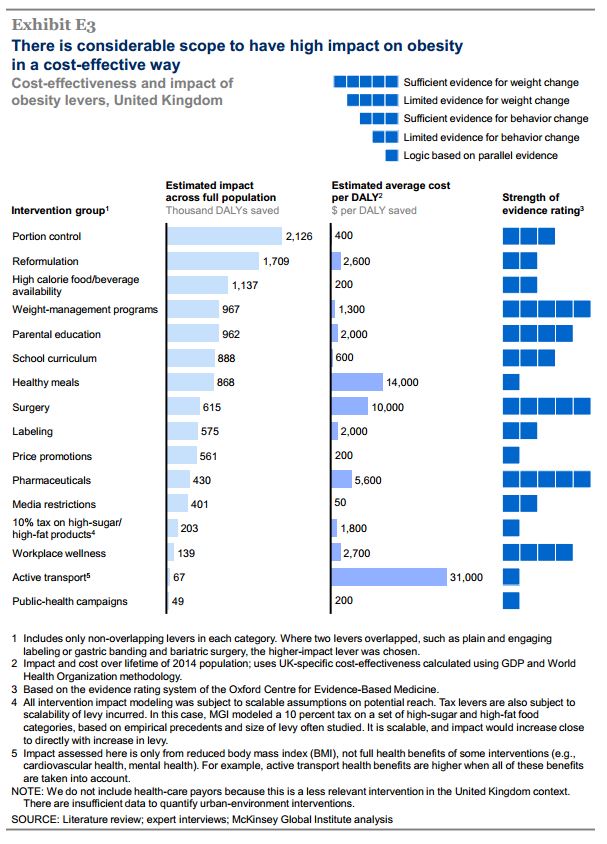
A new McKinsey Global Institute (MGI) discussion paper,Overcoming obesity: An initial economic analysis, seeks to overcome these hurdles by offering an independent view on the components of a potential strategy. MGI has studied 74 interventions (in 18 areas) that are being discussed or piloted somewhere around the world to address obesity, including subsidized school meals for all, calorie and nutrition labeling, restrictions on advertising high-calorie food and drinks, and public-health campaigns. We found sufficient data on 44 of these interventions, in 16 areas.
Although the research offers an initial economic analysis of obesity, our analysis is by no means complete. Rather, we see our work on a potential program to address obesity as the equivalent of the maps used by 16th-century navigators. Some islands were missing and some continents misshapen in these maps, but they were still helpful to the sailors of that era. We are sure that we have missed some interventions and over- or underestimated the impact of others. But we hope that our work will be a useful guide and a starting point for efforts in the years to come, as we and others develop this analysis and gradually compile a more comprehensive evidence base on this topic.
We have focused on understanding what it takes to address obesity by changing the energy balance of individuals through adjustments in eating habits or physical activity. However, some important questions we have not yet addressed require considerable further research. These questions include the role of different nutrients in affecting satiety hormones and metabolism, as well as the relationship between the gut microbiome and obesity. As more clarity develops in these research areas, we look forward to the emergence of important insights about which interventions are likely to work and how to integrate them into an antiobesity drive.
The main findings of this discussion paper include:
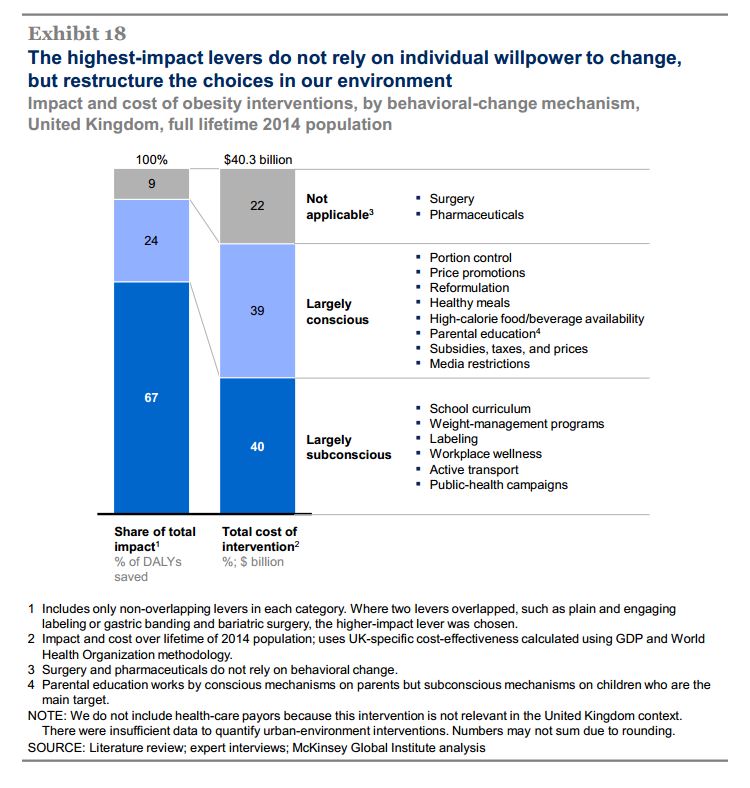
Existing evidence indicates that no single intervention is likely to have a significant overall impact. A systemic, sustained portfolio of initiatives, delivered at scale, is needed to reverse the health burden. Almost all the identified interventions (exhibit) are cost effective for society—savings on healthcare costs and higher productivity could outweigh the direct investment required by the intervention when assessed over the full lifetime of the target population. In the United Kingdom, for instance, such a program could reverse rising obesity, saving the National Health Service about $1.2 billion a year.
Education and personal responsibility are critical elements of any program aiming to reduce obesity, but they are not sufficient on their own. Other required interventions rely less on conscious choices by individuals and more on changes to the environment and societal norms. They include reducing default portion sizes, changing marketing practices, and restructuring urban and education environments to facilitate physical activities.
No individual sector in society can address obesity on its own—not governments, retailers, consumer-goods companies, restaurants, employers, media organizations, educators, healthcare providers, or individuals. Capturing the full potential impact requires engagement from as many sectors as possible. Successful precedents suggest that a combination of top-down corporate and government interventions, together with bottom-up community-led ones, will be required to change public-health outcomes. Moreover, some kind of coordination will probably be required to capture potentially high-impact industry interventions, since any first mover faces market-share risks.
Implementing an obesity-abatement program on the required scale will not be easy. We see four imperatives: (1) as many interventions as possible should be deployed at scale and delivered effectively by the full range of sectors in society; (2) understanding how to align incentives and build cooperation will be critical to success; (3) there should not be an undue focus on prioritizing interventions, as this can hamper constructive action; and (4) while investment in research should continue, society should also engage in trial and error, particularly where risks are low.
Exhibit
Cost-effective interventions to reduce obesity in the United Kingdom include controlling portion sizes and reducing the availability of high-calorie foods.
Enlarge
The evidence base on the clinical and behavioral interventions to reduce obesity is far from complete, and ongoing investment in research is an imperative. However, in many cases this requirement is proving a barrier to action. It need not be so. Rather than wait for perfect proof of what works, we should experiment with solutions, especially in the many areas where interventions are low risk. We have enough knowledge to do more.
About the authors
Richard Dobbs,James Manyika, and Jonathan Woetzel are directors of the McKinsey Global Institute, where Corinne Sawers is a fellow and Fraser Thompson is a senior fellow; Peter Child is a director in McKinsey’s London office; Sorcha McKenna is a principal in the Dublin office; and Angela Spatharou is a principal in the Mexico City office.