When working with raw data we’re often encouraged to present it differently, to give it a form, to map it or visualize it. But all maps lie. In fact, maps have to lie, otherwise they wouldn’t be useful. Some are transparent and obvious lies, such as a tree icon on a map often represents more than one tree. Others are white lies – rounding numbers and prioritising details to create a more legible representation. And then there’s the third type of lie, those lies that convey a bias, be it deliberately or subconsciously. A bias that misrepresents the data and skews it towards a certain reading.
It all sounds very sinister, and indeed sometimes it is. It’s hard to see through a lie unless you stare it right in the face, and what better way to do that than to get our minds dirty and look at some examples of creative and mischievous visual manipulation.
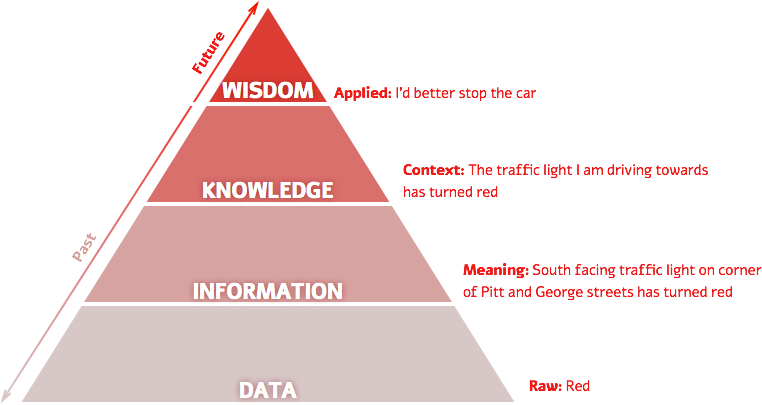
Over the past year I’ve had a few opportunities to run Disinformation Visualization workshops, encouraging activists, designers, statisticians, analysts, researchers, technologists and artists to visualize lies. During these sessions I have used the DIKW pyramid (Data > Information > Knowledge > Wisdom), a framework for thinking about how data gains context and meaning and becomes information. This information needs to be consumed and understood to become knowledge. And finally when knowledge influences our insights and our decision making about the future it becomes wisdom. Data visualization is one of the ways to push data up the pyramid towards wisdom in order to affect our actions and decisions. It would be wise then to look at visualizations suspiciously.
Centuries before big data, computer graphics and social media collided and gave us the datavis explosion, visualization was mostly a scientific tool for inquiry and documentation. This history gave the artform its authority as an integral part of the scientific process. Being a product of human brains and hands, a certain degree of bias was always there, no matter how scientific the process was. The effect of these early off-white lies are still felt today, as even our most celebrated interactive maps still echo the biases of the Mercator map projection, grounding Europe and North America on the top of the world, over emphasizing their size and perceived importance over the Global South. Our contemporary practices of programmatically data driven visualization hide both the human brains and eyes that produce them behind data sets, algorithms and computer graphics, but the same biases are still there, only they’re harder to decipher.
Remember that TED talk from a couple of years ago on texting patterns to a crisis hotline? The TED talker Nancy Lublin proposed the analysis of these text messages to potentially help the individuals texting. Her group, the Crisis Text Line, plans to release anonymized aggregates in the coming months.
Ms. Lublin said texts also provided real-time information that showed patterns for people in crisis.
Crisis Text Line’s data, she said, suggests that children with eating disorders seek help more often Sunday through Tuesday, that self-cutters do not wait until after school to hurt themselves, and that depression is reported three times as much in El Paso as in Chicago.
This spring, Crisis Text Line intends to make the aggregate data available to the public. “My dream,” Ms. Lublin said, “is that public health officials will use this data and tailor public policy solutions around it.”
People who lose or maintain weight in the long term are more likely to see distinct weight fluctuations over the course of a week than those who gain weight in the long term, according to a Finnish study.
The study, published in Obesity Facts, examined the weight of 80 adults across a week and how it related to their overall pattern of weight gain, maintenance or loss.
The researchers, from the VTT Technical Research Centre of Finland, in collaboration with Cornell University and Tampere University of Technology, found that there was an overall pattern of higher weight on Sundays and Mondays. However, those who lost or maintained their weight tended to lose more weight from Tuesday until the weekend than those who gained weight.
“Weight gain following a weekend can be thought of as normal weight variation,” said VTT research scientist Anna-Leena Orsama. “Some indulging during weekends and gaining a bit of weight isn’t harmful from the weight management point of view as long as this is compensated by healthy food choices during the week. It is important to notice these rhythms and take steps to reverse the upward trend after the weekend.”
The minimum monitoring period for participants’ weight was 15 days and the maximum was 330 days. Groups maintaining or losing weight managed to compensate for slight weight gain at the weekend, with weight decreasing from Tuesday until Friday, and the lowest weight frequently measured on a Friday or Saturday. However, those who gained weight overall had a less linear pattern, with minimum weight measured on all days of the week.
“It appears that long-term habits make more of a difference than short-term splurges,” the researchers wrote.
“Based on the findings of this study, we can expect weight to rise during weekends and treat it as a normal variation. Our results provide scientific support to the tenet that in weight management, allowing more flexibility during weekends and holidays might be more realistic and successful in the long term than a strict regimen.”
“No longer do people want to use technology as a synonym for a fax,” Bosch said. “But healthcare is very scared; we’re scared to develop on our own. If you look at any other industry, they have a huge research and development technology arm. Healthcare wants to manage technology like you’d manage a couple of horses in the stable. We’ll care for them and feed them, but we wouldn’t’ dare do anything else on our own. We’ve got to change our mindset.”
With patient engagement tools like Fitbit and personal health records growing more and more abundant, a primary goal of providers in today’s society must be to avoid obstructing the flow of information from patients and their tools to medical professionals, according to Ryan Bosch, chief medical information officer at Falls Church, Va.-based Inova Health System.
Bosch, speaking on a patient engagement panel at the Office of the National Coordinator for Health IT’s annual meeting in Washington, D.C., last week, called interoperability paramount to those efforts, but also called the health industry, as a whole, scared to innovate.
“No longer do people want to use technology as a synonym for a fax,” Bosch said. “But healthcare is very scared; we’re scared to develop on our own. If you look at any other industry, they have a huge research and development technology arm. Healthcare wants to manage technology like you’d manage a couple of horses in the stable. We’ll care for them and feed them, but we wouldn’t’ dare do anything else on our own. We’ve got to change our mindset.”
Part of changing that mindset, according to Donna Cryer–a D.C.-based patient advocate who suffers from autoimmune conditions–is thinking of patient care as more of a partnership. While Cryer said that she thinks of herself as both an engaged and an activated patient, she stressed that not all patients are willing or ready to take that same kind of initiative.
“A consumer might be someone who doesn’t have very frequent interactions with the healthcare system,” Cryer said. “I think it’s important to design education and engagement strategies and expectations for patients trying prevent hospital visits,” in addition to patients like herself who need constant treatment.
“Patient engagement takes at least two parties, and unless there’s that partnership, there really won’t be any engagement.”
Lygeia Ricciardi, director of the office of consumer eHealth at ONC, agreed, saying that patients need to feel comfortable asking questions and sometimes disagreeing with their providers. Technology, she added, helps to bridge a gap.
“If we can get information flowing to people, we want them to have a variety of tools and apps to work with,” Ricciardi said. “Trust is the bedrock of the patient-provider relationship. Patients must feel comfortable that their information is where it should be.”
Working with patients to achieve a common understanding of the types of information patients would be sharing, how the sharing would take place and which members of the clinical team would be reviewing the information and how often
Designating and training a member of the clinical care team to monitor incoming data and triage as necessary
Putting a medical emergency protocol in place
Using appropriate judgment in deciding when patient-generated electronic health information would be included in the physician’s legal medical record
The study focused on efforts within Project HealthDesign, a research program funded by Robert Wood Johnson Foundation.
Some see this as an opportunity to mobilise a peer-to-peer health knowledge commons outside the healthcare system that is filtered through government, hospitals and GPs’ surgeries. This new healthcare system would exist out among the public.
Pioneered by Tedmed’s clinical editor, Wellthcare tries to pinpoint the new kind of value that this people-powered healthcare system would create.
“Wellth” is closer to the idea of wellbeing or wellness than health; it is about supporting “what people want to do, supported by their nano-networks”.
A healthcare system that uses data we collect about ourselves would require these new bodies to make much bigger choices about how NHS trusts procure products and services.
Going back to the ever expanding market for wearable technology – with a potential patient group of 80m, there should be a lot more going on to turn our physiological data in the treasure trove it could be. Forget supermarket reward points and website hits, the really big data only just arrived.
Can we make the rise of wearable technology a story about better health for everyone, not just better gadgets for me?
Smartphone app visualises two similar running routesI am obsessed with my running app. Last week obsession became frustration verging on throw-the-phone-on-the-floor anger. Wednesday’s lunchtime 5km run was pretty good, almost back up to pre-Christmas pace. On Friday, I thought I had smashed it. The first 2km were very close to my perennial 5 min/km barrier. And I was pretty sure I had kept up the pace. But the app disagreed.As I ate my 347 calorie salad – simultaneously musing on how French dressing could make up 144 of them – I switched furiously between the two running route analyses. This was just preposterous; the GPS signal must have been confused; I must have been held up overtaking that tourist group for longer than I realised; or perhaps the app is just useless and all previous improvements in pace were bogus.My desire to count stuff is easy to poke fun at. It’s probably pretty unhealthy too. But it’s only going to be encouraged over the next few years. Wearable technology is here to stay. Smart phone cameras are also heart rate monitors. Contact lenses can measures blood sugar. And teddy bears take your temperature. A 2011 market assessment, estimated that there will be 80m sports, fitness and “wellness” wearable devices by 2016.
At the moment, it’s difficult to retrieve the data these systems collect. Nike only allow software developers access to data produced by people like me so they can create new features for their apps. I cannot go back and interrogate my own data.
Harbouring user data for product development is an extension of part of the search engine or mobile provider business model. When you log in to Gmail while browsing the internet, you give Google data about your individual search behaviour in exchange for more personalised results. Less obviously, when you use the browser on your phone, mobile companies collect (and sell) valuable data about what you are looking for and where you are. The latest iteration of this model is Weve, providing access to data about EE, O2 and Vodafone customers in the UK.
After Friday lunchtime’s outburst, I accepted that I’d never find the cause of my wayward run and quickly got absorbed back into the working day.
But I shouldn’t have.
We talk about the economic and social value of opening up government data about crime numbers or hospital waiting times. But what about the data we’re collecting about our daily lives? This is not just a resource for running geeks to obsess over, it provides otherwise unrecorded details of our daily lives. Sharing data about health has the potential to be an act of generosity and contribution to the public good.
For some areas of healthcare, particularly for type 2 diabetics or those with complex cardiovascular conditions, lifestyle information could make a huge difference to how we understand and treat patients. It could provide the kind of evidence badly needed to make headway in areas where clinical trials aren’t enough.
But it’s not yet easy to make something of this broader value created by fitness apps or soft toys with sensors in them. One person’s data is saved in different ways through different services – making for a messy, distributed dataset.
There is also no clear way to incorporate this into the current healthcare system. Some companies have made strides in that direction. Proteus Digital Health offers a system for monitoring a patient’s medication and physical activity using an iPad app and ingestible pills. This takes some much needed steps towards understanding how people comply with their prescription. At the moment, only 50% of patients suffering from chronic diseases follow their recommended treatment. If Proteus starts to sell information back to the health service, it will take digital health into mainstream healthcare. However,it hasn’t reached that point yet. And it is still a rare example of a company with the regulatory approval to do so. For example, Neurosky’s portable EEG machines, which measure brain activity, make excellent toys. But the company has no intention of certifying its products as medical equipment, given the time and expense it requires.
But does that matter? Neurosky’s wizard-training game Focus Pocus improves a player’s cognitive abilities including memory recall, impulse control, and the ability to concentrate. Some US medical practitioners are now prescribing Focus Pocus. This makes biofeedback therapy to ADHD patients available at home, replacing two to three hospital visits a week. This is going on anyway – outside the mainstream healthcare system.
Some see this as an opportunity to mobilise a peer-to-peer health knowledge commons outside the healthcare system that is filtered through government, hospitals and GPs’ surgeries. This new healthcare system would exist out among the public. Pioneered by Tedmed’s clinical editor, Wellthcare tries to pinpoint the new kind of value that this people-powered healthcare system would create. “Wellth” is closer to the idea of wellbeing or wellness than health; it is about supporting “what people want to do, supported by their nano-networks”. There is the potential for a future where we move from producers of data that is sucked up by companies into producers of data who consciously share it with one another, learn to interpret it and make judgments from it ourselves.
The current healthcare system may evolve to support this kind of change. In the UK, Academic Health Science Networks and Clinical Commissioning Groups provide new structures within the NHS that have the potential to support disruptive innovations. But so far these have led to small, incremental changes. A healthcare system that uses data we collect about ourselves would require these new bodies to make much bigger choices about how NHS trusts procure products and services.
Going back to the ever expanding market for wearable technology – with a potential patient group of 80m, there should be a lot more going on to turn our physiological data in the treasure trove it could be. Forget supermarket reward points and website hits, the really big data only just arrived.
Those pouring money into health-related mobile gadgets and apps believe they can work the miracle of making health care both better and cheaper
WHEN Kenneth Treleani was told last summer that he was suffering from high blood pressure, his doctor prescribed medicine to tackle the condition. He also made another recommendation: that Mr Treleani invest in a wireless wrist monitor that takes his blood pressure at various times during the day and sends the data wirelessly to an app on his smartphone, which dispatches the readings to his physician. Mr Treleani says the device (pictured), made by a startup called iHealth, has already saved him several visits to the doctor’s surgery.
Portable blood-pressure monitors have been around for a while. But the idea of linking a tiny, wearable one to a smartphone and a software app is an example of how entrepreneurs are harnessing wireless technology to create innovative services. By letting doctors and carers monitor patients remotely, and by making it simpler to collect vast amounts of data on the effectiveness of treatments, the mobile-health industry, or m-health as it has become known, aims to drive down costs while improving results for patients.
Many experiments are already under way in emerging markets, where new mobile devices and apps are helping relieve pressure on poorly financed and ill-equipped clinics and hospitals. But the biggest prize is America, which splashes out a breathtaking $2.8 trillion each year on a health-care system riddled with inefficiencies. The prospect of revolutionising the way care is delivered there is inspiring entrepreneurs. Mercom Capital Group, a consulting firm, reckons that of the $2.2 billion venture capitalists put into health-care startups last year, mostly in America, $564m went to m-health businesses.
The m-health market can be broken down into two broad categories. First, there are the apps and appliances used to monitor the wearer’s physical fitness. Firms such as Nike, Fitbit and Jawbone make wristbands and other wearable gadgets full of sensors that let people record their performance, and their calorie-burning, as they pound the pavement or sweat in the gym.
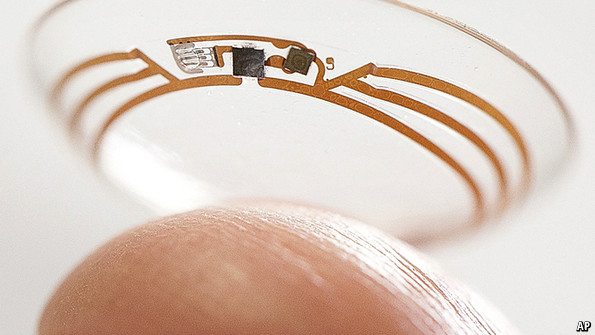
Second, other apps and devices link patients with a medical condition to the health-care system. Last month Google said it was working on a contact lens containing a tiny wireless chip and sensors that would measure and transmit the glucose levels in a diabetic patient’s tears. In December Apple was granted an American patent on a means to incorporate a heartbeat sensor into its devices.
Keeping an eye on glucose levels
The fitness apps may help people to keep up their training regimes, and in time make the population healthier. But in the shorter term they will not have much effect on the health-care system. Nor may they make many investors rich. IMS Health, a research firm, says that of the 33,000-plus health-related apps on Google Play’s app store (the figure for Apple’s iTunes is over 43,000), just five of them—of which two are calorie-counters—account for 15% of all downloads.
A growing posse of entrepreneurs think the big money is to be made in the second category, of apps and devices that seek to transform the way health care is delivered. Large companies spy an opportunity here too. Qualcomm, which sells wireless technology and services, has set up an m-health division, Qualcomm Life, and built a technology platform to make it easy for m-health companies to combine data about things such as the medicines people take and the results of tests they run on themselves, so their doctors can get a more complete picture of their health.
Among those firms with products already for sale, AliveCor makes a $199 gadget that attaches to a smartphone and lets patients take an electrocardiogram by placing two fingers on metal plates. It also sells a veterinary version for taking pets’ ECGs. The data are displayed in an app on the phone and can be reviewed (for a fee) by a cardiologist. CellScope, another startup, makes an otoscope—a device for looking inside the ear—that can be attached to an iPhone and an app that can send the images it takes to a physician.
Last year Medtronic, a huge medical-devices company, splashed out $200m to buy Cardiocom, which combines telehealth services with wireless home gadgets, including scales for heart patients for whom sudden weight gain may be a dangerous symptom. In October Verizon, a mobile-telecoms operator, launched a platform to transmit data from home devices, such as glucose monitors, to the firm’s secure “cloud” of servers.
As Don Jones of Qualcomm Life puts is, just as a car’s electronics tell a driver about its condition, so m-health devices and apps “give people dashboards, gauges and alarm signals” that make it easier for them and their doctors to track what is happening with their bodies. This may alert them to the need for action well before the patient’s condition deteriorates to the extent that he needs hospital treatment. Given that in America the average cost of a night’s stay in hospital is almost $4,300, there is scope for significant savings.
Another obvious way to use the technology to avert health crises is by checking that patients are taking their medicines. Propeller Health sells a device that fits on top of asthma inhalers, to monitor their use. Proteus Digital Health, which raised $63m last year, is testing an ingestible sensor that is taken at the same time as prescribed medication. The device, which relies on stomach fluids to complete a circuit to power it, transmits information to a smartphone so doctors and carers can track when a patient takes pills.
Again, the goal is to save money while improving health. The average annual cost of, say, treating sufferers from high blood pressure who fail to take their medicines is nearly $4,000 more than the cost of treating those who pop their pills reliably.
If such products live up to their promise, a side-effect may be that there is less need for medical technicians—an example of a wave of technology-related job losses that some economists expect. The development of machine intelligence, another hot area for investment (see article), may eventually mean there is less need for doctors or specialists to analyse test results.
One snag is that techies’ enthusiasm for such innovation is colliding with the health-care industry’s conservatism. Doctors in America have been paid for delivering more care, so products that might lead to fewer billable patient visits are viewed with suspicion. This is changing gradually as insurers switch towards rewarding hospitals for providing a better quality of care instead of simply paying them for the quantity delivered. But there is a long way to go in making the medical profession take an interest in cost-saving: a study last month in Health Affairs, a journal, found that few American surgeons had any idea of the cost of the devices, such as replacement hip joints, they implant in patients.
Encouraging iPochondria
Insurers may have cause to worry that, instead of reducing doctors’ workloads, the spread of m-health devices and apps may only encourage hypochondria: surgeries may be flooded with the “worried well”, fussing over every slightly anomalous reading. That may keep the medical profession nicely busy, but will not curb the ever-rising cost of health care.
So, to win over doctors, hospital managers and insurers, m-health firms will need to gather evidence to support their claims of cost-cutting and improved patient outcomes. Such evidence is still surprisingly scarce, says Robert Kaplan of the National Institutes of Health, a government agency. Stephen Kraus of Bessemer Venture Partners, which has examined hundreds of m-health startups, says many firms are blithely assuming that all you have to do is “appify” health care and the world will change.
Makers of more sophisticated m-health products, aimed at doctors, clinics and hospitals rather than patients, will have to build a sales force like that of a pharmaceuticals company, says Bob Kocher of Venrock, another venture-capital firm. That will take time and lots of money.
Some m-health products may have to win approval from America’s Food and Drug Administration. Most firms were pleased by a plan the FDA published last year that said it would regulate only those m-health products that do the work of a traditional medical device—an ECG, say, but not a pedometer. But applying for approval is still burdensome. And the FDA has not finished drawing up its rules: m-health firms are waiting for a framework on the use of information technology in health care from the FDA and two other agencies. Despite such obstacles, optimists such as Peter Tippett of Verizon see health care undergoing the mobile transformation that banking and other industries have already been through.
Andrew Thompson, Proteus’s boss, hopes that the sensors and software his firm is developing will form the dominant “platform” for m-health in the way that Facebook dominates social networking and lets other firms build apps that run on it. But it is likely to face stiff opposition. Mr Kocher thinks giants like Google and Apple may seek to build m-health platforms too.
Apple filed its patent for a “seamlessly embedded heart-rate monitor” after looking for ways to replace passwords with biometric methods—in this case, an ECG—to authenticate users. It may think carefully before entering a business as heavily regulated as medical devices. But it has made no secret of its interest in selling wearable gadgets packed with sensors; and if consumers prove as keen on m-health as investors currently are, it will surely want to satisfy them.
Firms that aspire to make serious money in m-health will need plenty of patience and deep pockets. But they may be able to rely on an army of technophile patients who lobby their doctors to incorporate the new devices and apps in their treatment programmes. Mr Treleani is one of them: “I’d be suspicious of medical practices that aren’t moving forward with these new technologies,” he says.
“If you want to change some behavior, whether it’s flossing your teeth, eating more fruits and vegetables, or getting more exercise, keeping a record of that behavior is a sensible place to start,” says Blair.
The activity tracker without counseling wasn’t enough. Only those who wore the tracker and received group and telephone counseling lost more weight—about 13 pounds more—than the control group.
Rupert Murdoch wears one on his left wrist. “This is a bracelet that keeps track of how I sleep, move, and eat—transmitting that information to the cloud,” the international media mogul told an audience in Sydney, Australia, last November.
“It allows me to track and maintain my health much better.”
Personal activity trackers—like the Jawbone Up, Fitbit Flex, and Nike+ Fuelband—are the latest personal fitness gadgets.
“Some of them, like the BodyMedia armband, measure total energy expenditure, as well as intensity of activity and bouts of activity,” says Steven Blair, professor of exercise science at the University of South Carolina.
“If you sit for 10 minutes, and then get up and walk for one minute, it detects the different intensities and durations,” Blair explains. “It’s a more complex device that gets us closer to the truth than simple pedometers or accelerometers.”
Are activity trackers worth their price tag—from $10 for a step counter to over $100 for a more sophisticated armband?
“If you want to change some behavior, whether it’s flossing your teeth, eating more fruits and vegetables, or getting more exercise, keeping a record of that behavior is a sensible place to start,” says Blair.
A recent study hinted that activity trackers might help people lose weight.
Blair and his colleagues enrolled 197 overweight or obese middle-aged adults in a weight-loss program for nine months. Fifty received only a weight-loss manual (they were the control group), 49 got the manual plus an activity tracker to wear, 49 got the manual plus counseling sessions but no tracker, and 49 got the manual, the counseling, and the tracker.
The activity tracker without counseling wasn’t enough. Only those who wore the tracker and received group and telephone counseling lost more weight—about 13 pounds more—than the control group.
But for people who just want to know how physically active they are, “it’s not necessary to have a really complicated and sophisticated device,” notes Blair.
“A simple pedometer could tell you how many steps you’re getting. And if you’re getting 3,000 per day and you know that’s not enough, you can set a realistic goal of 1,000 more. And next week you can check to see whether you met that goal.”
Source: Int. J. Behav. Nutr. Phys. Act. 2011. doi:10.1186/1479-5868-8-41.
The point isn’t the gadget: it’s the combination of the intimacy of a device that is always with us and that only we use, with the power of cloud-based processing and storage. The wearable device itself is actually only the small, physical manifestation of a much larger service: Google Glass gives its wearers a head-up display, voice control and a forward-facing camera, but it’s only through a connection to the internet that it can live up to its potential
“He put this engine into our ears,” wrote the Lilliputians, in Gulliver’s Travels, Jonathan Swift’s 1726 classic, “which made an incessant noise, like that of a water-mill: and we conjecture it is either some unknown animal, or the god that he worships; but we are more inclined to the latter opinion, because he assured us, (if we understood him right, for he expressed himself very imperfectly) that he seldom did any thing without consulting it. He called it his oracle and said it pointed out the time for every action of his life.”
Just as Gulliver’s Travels was a satire, and its description of his watch essentially a tease on time-based affairs, so too we are starting to find that the accoutrements of our modern communications are ripe for mickey-taking. The Bluetooth headset has gone from a status symbol to the mark of a tosser. There’s a Britishness to this — a who do you think you are to need such a device? thing. There’s also a feeling of enslavement that might be hard to shake. Just as our culture turns towards reducing the digital distraction in our lives, will we really want to be cuffed to our inbox? It’s said that in a ham-and-egg sandwich, the chicken is involved but the pig is committed: just how committed to our communications do we want to — or want to appear to — actually be?
“It’s not information overload. It’s filter failure.” Clay Shirky
This article was taken from the January 2014 issue of Wired magazine. Be the first to read Wired’s articles in print before they’re posted online, and get your hands on loads of additional content bysubscribing online.
Wearables are truly upon us. It takes about a decade to shift: from the basements of the 70s, to the desks of the 80s, the laps of the 90s, the front rooms of the noughties and pockets of the twenty teens, the location of hot computing — the place where the most interesting developments are happening — always moves and shrinks with every generation. And although this decade is all about the smartphone, today we’re starting to see the path to the next stop in this constant progression: if not in, then definitely on the body.
As we’ll discuss, this leap, from the situated and leave-behindable to the always-on, always-present, always–connected, is not without its drawbacks. But it also promises a near-future world of self-knowledge, sensors and superpowers. Even today we can monitor our activities and compare ‘n’ share with our friends via devices such as the Nike+ FuelBand, the Fitbit or the Jawbone UP; and we can bring information, alerts and alarms to our wrist with devices like the Pebble watch. Coming devices will give you head-up displays, vibrating interfaces, speech recognition and a constant –understanding of where you and it are in time and space. By smearing the interface between –yourself and the internet across your nervous system, wearables are the first step in augmentation of the human. They give us superpowers in the same way cybernetic implants do to the heroes of science fiction.
The point isn’t the gadget: it’s the combination of the intimacy of a device that is always with us and that only we use, with the power of cloud-based processing and storage. The wearable device itself is actually only the small, physical manifestation of a much larger service: Google Glass gives its wearers a head-up display, voice control and a forward-facing camera, but it’s only through a connection to the internet that it can live up to its potential.
And what potential — never forget a name again, thanks to its camera, facial-recognition tech and a link to your social networks. Never be lost, through the map hovering in the corner of your eye. Develop an instant expertise in the art you’re looking at with a reverse image-search and a Wikipedia lookup. Have perfect memories of everything you do, say, see or hear through a constant archive of point-of-view shot from your forehead. Be a more scintillating conversationalist by recording, transcribing and automatically Googling everything you hear. Link your devices and adjust your day’s agenda to match your pulse-rate-monitored stress levels. Receive an ambient alert to your wrist whenever you’re close to something that’s on your phone-stored shopping list, and whisper to your glasses to show you where it is on the shelf. Feel a tingle in your pocket when you walk past someone whose OKCupid profile matches your own, and whose biomonitoring devices -indicate is in a receptive mood. Automatically plot a route to work that takes you past breakfast places whose menus match your immediate biochemical needs, and have this hover in front of you as you cycle, with warnings for when you’re pedalling too hard for your heart, and notifications of upcoming meetings being cancelled, as you sub-vocalise acknowledgements in English, having them translated in real-time into the Japanese of your colleague’s wrist-bound diary.
Many of these scenarios are dependent on different devices, from different manufacturers, successfully talking to each other: for wearables to sing the body electric, they must first form choirs. Rival firms will have to adopt compatible standards and allow for truly open development before the more advanced ideas are possible. But these are engineering and business decisions. More important for wearables, with their curious mix of the intimate and the public, is the social reaction to their use.
The surest sign of a technological niche about to be filled is an outbreak of Apple rumours. No other firm produces such a flurry of speculation, guesswork and extrapolation of minor signals as Apple. The iWatch (name by popular consensus) has never been mentioned by anyone from Apple, nor has anyone from its supply chain spoken of it or leaked any details, but nevertheless there are signs that such a thing might be on its way.
Apple has a handful of patents that look useful, plus there are a few details in the new iPhone and iOS that would make a lot of sense if an iWatch existed. The iPhone 5s has a chip dedicated to monitoring its owner’s movements, making it in essence a pocket-carried FuelBand, which shows that Apple is at least paying attention to the quantified-self idea. And iOS7 has a feature, iBeacon, which allows for communication with low-powered devices using the newest Bluetooth standard. That would be very useful over the range between your pocket and your wrist. Siri, the voice interface on iOS, would be splendid on a wearable, and the iOS notifications screen looks eminently transferable. But all of this is, of course, entirely conjecture. The beguiling/tiring axis of Apple product fantasies is subject to the traditional Apple announcement-and-launch schedule, and the likely slot for the Next Big Thing is the mid-January keynote, just in time to make everyone look mournfully at their month-old but now painfully past-it Christmas presents.
Like many internet technologies, wearables are very much a product of the environment in which they are funded and designed, primarily that of Silicon Valley — both the physical place and its thought-construct offshoots around the world. Invariably, the use-case scenarios for wearables both address problems that are two degrees away from behaviours not already invested in, and furthermore take a technofundamentalist position on existing social norms.
To think about this, consider that there are two classes of wearables today: the introspective, which monitors what you do and where you go, and informs you of changes to the state of your body and expanded self in cyberspace; and the extrospective, which looks outwards, to monitor and record the world around you. A Nike+ FuelBand is introspective. A Narrative Clip cam, which takes pictures constantly as you wear it, is extrospective. The introspective is of no concern to others. Who cares if you’re counting your steps? But the extrospective is a different beast. Society has yet to evolve the correct etiquette for having a meeting with someone who is constantly recording and archiving their conversations, or for going to a party with someone whose necklace is uploading pictures of you to the cloud every 30 seconds. It is as hard to imagine future generations’ views on these things as it is today to understand the Victorians’ erotic desire for table legs. But today’s society might find it challenging, if not already illegal, under different countries’ privacy laws. You may be able to remember the faces of all the people you meet, but use a device to capture them automatically and put them into a database, and a line is being crossed — even if that data is inaccessible to others. Whether that line demarcates violating others’ privacy — or breaking your own sense of non-augmented humanity — is something we will have to hash out.
Some wearable technology has already developed a level of understood etiquette. A glance at your watch in the middle of a meeting is rude. But it’s also an action that is understood by the person you are meeting: you wanted to know the time. Wearables, especially those with displays that cannot be seen by others, go much further than this. You may be aware that the other person just interacted with their device, but you have no idea what that interaction was. As interfaces become more ambient, or more fluid, the social meaning of interacting with them mid-conversation becomes more confused and potent. Today’s one-on-one conversations might be tomorrow’s one-on-one-plus-her-fact-checking-AI conversations. Just what did that mid-conversation microdistraction mean? That your lies have been found out, or that their football team just scored? It will be unnerving.
Valley-based technologists, however, may take the more fundamentalist view that it is not their technologies’ place to deal with human insecurities, but rather society’s job. The ideology of what it is possible to do with the technology is paramount, and human squeamishness has no role to play: a sort of device-led fait accompli. This is already happening, for example, in the concerns expressed around the supposed inability of the digital world to forget youthful indiscretions, prompting the then CEO of Google, Eric Schmidt, to suggest that in the future, people might change their name at a certain age to reset their online identity. Wearables could accelerate this process.
The social and the technical are inevitably interlinked. Although wearables have themselves been enabled by advances in chip design and component miniaturisation, it is perhaps that relentless technological progress that precedes their downfall. There is an old joke in software design that all programs expand until they can receive email. Likewise, we might suspect that all tiny devices will upgrade until they are general–purpose computers. This has already happened with phones — the iPhone 5S is purportedly as powerful as a MacBook Pro from 2008 — but phones can be put away, or obviously turned off. A wristband that today might be expected to just count your steps could, in theory, be programmed to record all that happens around it, upload that data to the cloud and do something mysterious with it. We are never sure about how new technologies will be received, and history is full of examples of our willingness to accept new deskbound technologies. Wearables, –however, push tech into the fields of fashion, of social signifier and public display. At your laptop, in private, you’re hard to judge. Use these technologies in public, and they enter a different realm.
“He put this engine into our ears,” wrote the Lilliputians, in Gulliver’s Travels, Jonathan Swift’s 1726 classic, “which made an incessant noise, like that of a water-mill: and we conjecture it is either some unknown animal, or the god that he worships; but we are more inclined to the latter opinion, because he assured us, (if we understood him right, for he expressed himself very imperfectly) that he seldom did any thing without consulting it. He called it his oracle and said it pointed out the time for every action of his life.”
Just as Gulliver’s Travels was a satire, and its description of his watch essentially a tease on time-based affairs, so too we are starting to find that the accoutrements of our modern communications are ripe for mickey-taking. The Bluetooth headset has gone from a status symbol to the mark of a tosser. There’s a Britishness to this — a who do you think you are to need such a device? thing. There’s also a feeling of enslavement that might be hard to shake. Just as our culture turns towards reducing the digital distraction in our lives, will we really want to be cuffed to our inbox? It’s said that in a ham-and-egg sandwich, the chicken is involved but the pig is committed: just how committed to our communications do we want to — or want to appear to — actually be?
As timepieces, wristwatches have been generally replaced by the clock on your phone. But that notwithstanding, a cheap digital watch keeps the time as well as the most expensive chronometers. Spending more than £5 on a watch is not a decision of practical use: the men’s watch market, for example, is now almost entirely one of fashion, of signifiers of wealth, of male-accepted jewellery — either that, or wine bars are popular with deep-sea divers.
But that market is based entirely on notions of craftsmanship, tradition and symbols of supposed manliness that are notably absent with the sort of wearable technologies we’re talking about here. Equating rapidly innovating devices with luxury misses the point of either: you can stick jewels to something, or you can make it super rugged, but neither of those will take away from the fact that they are functional devices, soon to be declared obsolete and upgraded. They’re built to do a job; on the nature of that job will you be judged — and that job might be nerdy.
The slow roll-out of Google Glass is a case in point. It is undoubtedly amazing technology and there are plenty of use-cases for wearing it while doing something else. But even before anyone had seen it in the wild, there was a word for people wearing it casually around the place: “glassholes”. Already dubbed “a Segway for the face”, Google Glass may turn out to be the most useful thing ever, but wear it all the time and you’ll be put into the same social slot as people with shoulder-holsters for their BlackBerry.
Ultimately, though, that’s a question of marketing and the transformation of social norms. So too is our commitment to our data. The recent fashions of unplugging, digital detoxing, email fasts and screen-break sabbaths have highlighted the desire of many to be free from the constant flow of information. As an activity that happens in front of a large, special-purpose machine on our desks, this feels like work, even when it’s play.
The limitations of the devices might be their, and our, saviour in this regard. As NYU professor and writer Clay Shirky says, “It’s not information overload. It’s filter failure.” Perhaps the limited size of the display, the cruder signalling from a wearable device, will encourage developers to refine those filters. If all you can display is a few lines of text, or if it’s one vibration for left and two for right, then the filtering will need to be done by the system, and not by the user. The stupid device being the pointy end of complex software places the responsibility for technological sophistication back into the laps of the programmers and designers.
Wearable technologies promise a great deal. For the individual, their usefulness, their very intimacy, offers a levelling-up of personal ability and self–understanding. One app that already exists for the iPhone, Word Lens, offers real-time translation of printed text, such as street signs, in the video camera, laid over the original text. That or something like it will be a Google Glass app sooner or later.
The barrier between the internet and the rest of the world is weakened by wearables, and their technology is no longer a personal matter. Using them might prove to be — in circumstances of extrospection, or of massive–augmentation of personal ability — considered socially unacceptable, unfair or just uncool. How that social progress plays out will be just as interesting as the technology itself. Personal computing is no longer personal. We will wear it like we wear our heart: on our sleeve.
Rethinking Health: Introducing “HICCup” – A New Opportunity for Investing in the Health of Communities
Dear Paul Nicolarakis,
Sorry we missed you! Our records indicate that you registered for this webinar, but were unable to attend.We invite you to listen to the recording and download the slides at any time by clicking on the link to the right of this message.
Thank you again and we look forward to your participation in future QC Learning Community webinars!
Meeting Description:
What’s the return on the $3 trillion that we spend each year in the U.S. on health care? If we treated health care as an investment, a smart portfolio manager would invest a better part of this money into community health and prevention that could reduce the need for high-cost care in the first place.That’s the thinking behind HICCup (Health Initiative Coordinating Council), a new non-profit initiative with a mission to preserve and restore health at the community level. Founded by Esther Dyson, an active angel investor in health companies and launching in 2014, HICCup will work collaboratively to identify up to five small communities across the U.S. that will compete to win the “HICCup Prize” for the greatest cost-effective improvement in health (not health care) over five years. Together, HICCup will work with communities to create community marketplaces that refocus competition, business models and investment on better health with financial returns.
Join us to hear from Esther Dyson and Rick Brush of HICCup to learn more about this opportunity and share your ideas for Maine communities that are ready to create investable markets for the “production of health.”
Esther Dyson, founder of HICCup and chairman of EDventure Holdings, is an active angel investor, best-selling author, board member and advisor concentrating on emerging markets and technologies, new space and health. She sits on the boards of 23andMe and Voxiva (txt4baby), and is an investor in Crohnology, Eligible API, Keas, Omada Health, Sleepio, StartUp Health and Valkee, among others. Her sisters include a nurse who lives in Pownal, Maine, and a vet, a cardiologist and a radiologist.
Rick Brush
Rick Brush, executive director of HICCup and founder of Collective Health, is a former corporate strategist in health and financial services, including nearly a decade at the health insurer Cigna. He’s now focused on creating markets for health-impact investing. Collective Health’s project to reduce childhood asthma emergencies in Fresno, California, is laying the groundwork for the first Health Impact Bond in the U.S.
For more than three decades, the JP Morgan Healthcare Conference in San Francisco has been the almost-exclusive domain of pharmaceutical companies, the place where the Mercks and Pfizers of the world meet biotechnology startups who help them fill their pipelines.
But it’s a different world today, one where new laws and new digital technologies are upending the way health care is delivered.
Attendance at the conference has changed to reflect the new reality, as health-insurance companies, software developers, purveyors of big-data analytics and a range of other information technologies have begun to fill out the roster, on the presenters’ stages and in the nearby hotels where the deal-making happens.
“I’ve been coming to this for five years,” said Krishna Yeshwant, a general partner at Google Ventures, which backs a range of health- and health-information startups. “When I started it was all pharma, and all the talk was about disease targets.
“The Affordable Care Act has led to this shift, and has created a business model that didn’t even really exist five years ago. There is all this talk now about analytics, about digital health, health-care delivery. I have [portfolio company CEOs doing information-technology] who ask me, ‘Should I be going to JP Morgan?,’ and I say ‘Yes, you have to be here.’ A few years ago I might have said no.”
This year’s conference not only saw a fireside talk from Acting National Coordinator of Health I.T. Jacob Reider, but presentations from electronic health-record providers like Practice Fusion Inc. and athenahealth Inc.
The conference also featured a standing-room-only panel discussion with startup digital-health companies like medical-information network ShareCare Inc., “digital medicines” company Proteus Digital Health Inc. and big-data analytics company Kyruus Inc., joined by health IT investors Qualcomm Ventures and Thrive Capital. It was the first year digital health had gotten such prominent billing at the conference. JP Morgan organizers declined to comment about trends in conference attendance in recent years.
One provision of federal health reforms ties hospitals’ reimbursement for treatment more closely to patient outcomes than to the volume of patients treated.
Feeling more scrutiny, health-care providers now have an immediate need for the types of software and big-data products that can help them track treatment efficacy and patient progress over large populations of people, Dr. Yeshwant said.
“These kinds of products always made good sense,” he said, “but there was no real financial incentive. Now there is. If you’re not doing this, you’re going to disappear.”
More of a gradual change than an overnight transition, the “outcome-based medicine” provision of health-care reform has drawn a number of new players to the JP Morgan conference, including all of the country’s top health insurance companies and a range of IT providers who want to do business with them and with hospitals, Dr. Yeshwant said.
“Many of these people come because they want to be near the conversation,” he said. “Things are not changing abruptly, but these changes are very big. A lot of people feel the need to be near all of it.”
Google Ventures is backing a number of health information-technology companies, including genomic analysis company Foundation Medicine Inc., big data company DNANexus Inc. and consumer-genetics company 23andMe Inc.


 Smartphone app visualises two similar running routesI am obsessed with my running app. Last week obsession became frustration verging on throw-the-phone-on-the-floor anger. Wednesday’s lunchtime 5km run was pretty good, almost back up to pre-Christmas pace. On Friday, I thought I had smashed it. The first 2km were very close to my perennial 5 min/km barrier. And I was pretty sure I had kept up the pace. But the app disagreed.As I ate my 347 calorie salad – simultaneously musing on how French dressing could make up 144 of them – I switched furiously between the two running route analyses. This was just preposterous; the GPS signal must have been confused; I must have been held up overtaking that tourist group for longer than I realised; or perhaps the app is just useless and all previous improvements in pace were bogus.My desire to count stuff is easy to poke fun at. It’s probably pretty unhealthy too. But it’s only going to be encouraged over the next few years. Wearable technology is here to stay. Smart phone cameras
Smartphone app visualises two similar running routesI am obsessed with my running app. Last week obsession became frustration verging on throw-the-phone-on-the-floor anger. Wednesday’s lunchtime 5km run was pretty good, almost back up to pre-Christmas pace. On Friday, I thought I had smashed it. The first 2km were very close to my perennial 5 min/km barrier. And I was pretty sure I had kept up the pace. But the app disagreed.As I ate my 347 calorie salad – simultaneously musing on how French dressing could make up 144 of them – I switched furiously between the two running route analyses. This was just preposterous; the GPS signal must have been confused; I must have been held up overtaking that tourist group for longer than I realised; or perhaps the app is just useless and all previous improvements in pace were bogus.My desire to count stuff is easy to poke fun at. It’s probably pretty unhealthy too. But it’s only going to be encouraged over the next few years. Wearable technology is here to stay. Smart phone cameras 
 Keeping an eye on glucose levels
Keeping an eye on glucose levels