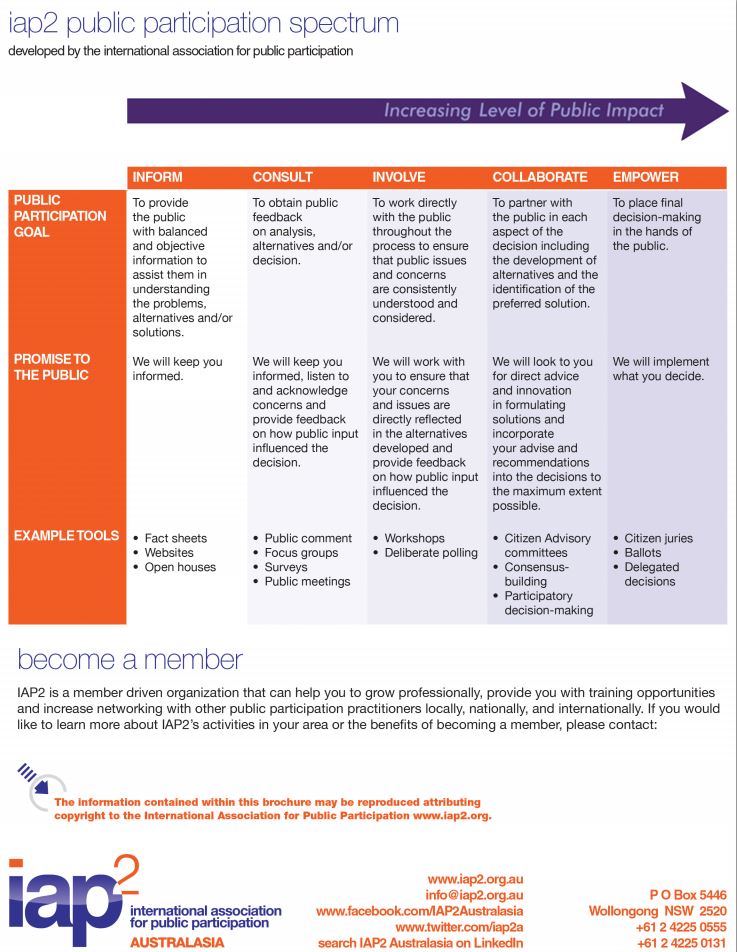
And so the slow, arduous public conversation task begins…
PDF: AFR_Healthcare20_BigDataRoundtable_140625
Story & Video: http://www.afr.com/p/business/healthcare2-0/leadership_vacuum_cripples_health_VrDsiSCDYOWXyuvg54QfJN
Leadership vacuum cripples e-health
PUBLISHED: 19 JUN 2014 05:36:14 | UPDATED: 20 JUN 2014 05:18:23

MARK EGGLETON
Australia continues to struggle with the concept of e-health, with numerous health sector stakeholders equally to blame. This was one of the key messages to come out of the recent Big Data in Healthcare roundtable held by The Australian Financial Review in partnership with GE in Sydney.
Capital Markets CRC principal adviser Dr Paul Nicolarakis suggested part of the problem was Australia lacks a vision for healthcare. He suggested we don’t have someone or a collection of individuals working towards one goal. There are numerous stakeholders across the sector all vying to be the loudest voice, yet not pursuing a common goal.
Chief scientist at The George Institute for Global Health, Professor Anushka Patel said there was no one out there explaining and selling the potential value of big data and e-health or really engaging the government in a productive manner.
“There’s potential to reduce waste and reduce healthcare expenditure without sacrificing quality of care and health outcomes,” Professor Patel said.
“I also think big data could improve our ability to ensure equity, better health outcomes and health access. Those are the two of the big policy messages that need to be conveyed.”
Professor Enrico Coiera, who is the director of the Centre for Health Informatics, said data is already on the move – it just needs to be better linked. He said there is already plenty of data that’s slowly improving quality out there.
“The job is to get that moving around the system. Cheap fees and hospitals sharing information is what we want. Importantly, let’s drop the e from e-health and just improve health services,” Professor Coiera said.
Paul Nicolarakis reiterated that part of the problem was we lack strong, informed, insightful leaders of our health system.
“With all respect to the Australian Medical Association, they are not appointed to be the leaders of the health system. Our health ministers are not health people, they aren’t clinicians or experts in health, and I think, because of these sort of structural limitations, it’s very hard to develop the idea of e-health.
THE TIME IS RIPE FOR CHANGE
For the head of the Australian Healthcare and Hospitals Association, Alison Verhoeven, the time is ripe for change right now. She suggested that, with the federal Health Minister Peter Dutton talking about structural reform in the health system, the time is right to really address the big data question as it can help drive efficiency.
Verhoeven said a more streamlined system would see better consumer as well as clinician engagement.
“It’s about better system leadership as well.
“I’d really like to see a more integrated healthcare system generally come out of the structural reforms being discussed at the moment but whether that happens or not is another matter,” she said.
GE Healthcare Solutions managing director Dr David Dembo shares Verhoeven’s cautious view that we’re not going to see any real change in Australia.
“Unfortunately change happens very slowly in health and it happens slowly because free market principles don’t apply and because we don’t have strong leadership.
“We need to have people step up to the plate who are prepared to make brave and considered decisions, particularly around selling a vision and building a culture that gets buy-in from everybody – doctors, consumers and politicians.
“This journey we’re going on to take the ‘e’ out of e-health is the opportunity to de-fragment our health system and you only do that when everybody agrees this is a data science and this is our opportunity for health to behave as a system.”
The Australian Financial Review
Story: http://www.afr.com/p/business/healthcare2-0/privacy_fears_curb_health_growth_kxxq9sVuxrKDFz6enebgWP
Privacy fears curb e-health’s growth
PUBLISHED: 15 HOURS 46 MINUTES AGO | UPDATE: 14 HOURS 8 MINUTES AGO

“We have to be able to sell people a vision about why e-health is important to them,”, says Australian Healthcare and Hospitals Association CEO Alison Verhoeven. Photo: Reuters
MARK EGGLETON
In a twist on the old highwayman demand of “Your money or your life” we finally have an answer when it comes to e-health. Our personal finances win while our health takes a back seat.
Right now most Australians when they want to get a snapshot of their financial situation can go online and find up-to-the-minute information on their bank balance and outstanding debts. We’re pretty comfortable with the level of security afforded our financial details and even happy to give out further details if we’re keen on purchasing goods or services. Unfortunately, we’re a little leery about having our health records available online beyond what’s stored in a computer on our GPs desk.
Security of data was one of the major focuses of the recent Big Data in Healthcare roundtable held byThe Australian Financial Review in partnership with GE in Sydney with most participants agreeing it was an issue.
According to Australian Healthcare and Hospitals Association CEO, Alison Verhoeven, the best way to address people’s privacy concerns is better communication.
“We have to be able to sell people a vision about why e-health is important to them,” she says.
Furthermore, Verhoeven worries that while we continue to argue around the fringes of the debate we’re falling behind as technology moves on.
“The focus of discussion around e-health is on the desktop versions of e-health. We haven’t actually really begun to talk about the mobile versions of e-health so we’re really constructing a system that works on old technology,” Verhoeven says.
Part of the problem with Australia’s roll-out of some form of e-health framework was the personally controlled electronic health record (PCEHR) set up by the last federal government was it was poorly conceived and advertised, with very few Australians opting to participate.
OPT OUT, NOT OPT IN
Chief scientist at The George Institute for Global Health, Professor Anushka Patel says the best option would have been to give Australians the opportunity to opt out of the PCEHR rather than opt in.
In her experience in health services research it’s often very difficult to get opt-in consent, logistically, and opt-out consent is frequently used.
“Very few people opt out. Even in situations where opt-out can occur later in the course of the investigations very few people opt out. That’s a real test of whether people have real concerns such as privacy. I certainly think opt-out is the way to go,” Professor Patel said.
Director of the Centre for Health Informatics Professor Enrico Coiera says people do have a right to be a little apprehensive about data security and part of the problem is health services, especially government departments, don’t really “have their heads around the issue yet”.
For Paul Nicolarakis, the principal adviser from Capital Markets CMC and former senior adviser to Tanya Plibersek (the previous government’s health minister), the privacy question is an obvious concern. Yet he believes we have communicated the benefits of e-health in the wrong way.
“If e-health is valuable then it’s the same conversation as immunisation. It’s like everyone feels a bit of pain, you’ve got to go get your injections, but there’s value, which is you don’t get sick.
“If we can start framing an e-health record, as immunisation has been so brilliantly framed over the years, then I think people will get it. The analogy runs right through to there even being a kind of herd immunity granted to the population when everyone or most people are on board. The upside for the community is massive, and I don’t think that’s been articulated that well,” Nicolarakis says.
Interestingly, the US, which a few years ago was in last place in terms of implementing an e-health strategy, is now considered a leader in terms of policy sharpness and ensuring e-health has a positive impact.
US EXAMPLE
The US has built the idea of “meaningful use” into the core of their electronic health record technology.
“It’s not talking about whether you have your boxes ticked in terms of what software you’ve got or what computers you have. It asks the question of whether the e-health record has a meaningful impact on patient care,” Nicolarakis says.
Dr Terry Hannan from the University of Tasmania and Launceston Hospital has seen the meaningful impact more connected health and better use of data can have on a number of projects around the world. He was the co-founder of the largest e-health system in the world for managing the AIDS epidemic of 40 million people in Africa.
“We’re now in over 200 countries in the world and we have a massive amount of standardised data for clinical day-to-day care, resource utilisation, research and outcomes. It’s now linked to the mobile health phenomenon and patients are using their own data via a mobile phone as a tool for improving their care.”
Hannan says similar programs have been rolled out in a number of communities in developing countries.
“In Pakistan, we track the multi-drug treatment for tuberculosis right down to the individual house and patient.
We can monitor the food that’s supplied to these impoverished people so they comply with their medication, all recorded on a mobile phone in a country with interrupted connectivity to the internet,” Hannan says.
PREVENTATIVE OPPORTUNITY
The roundtable panel agreed the great potential of e-health lies in the preventative health sphere where the use of non-health data such as our nutrition habits could help revolutionise our future health outcomes.
Professor Patel says we could potentially link the quite extensive databases that already exist.
“We already have one for everything that’s available in any supermarket in Australia and a lot of that information was crowd-sourced – people with their mobiles.
“Link that to frequent user, loyalty programs that some of the big supermarkets have and we can look at what people spend at the check-out counter, and you can very accurately predict how levels of obesity are going to change due to the composition of people’s diet, their salt intake and more,” she says
“It allows you to target health outcomes at the policy level.”
Unfortunately, this hardly gets mentioned in the more emotive debates around privacy and the supposed infallibility of clinicians.
“Most of the unexplained variation in health research is from people who believe their own clinical insights and experience is of greater value than what might be data driven or might be evidence-based,” Patel says.
Verhoeven agrees and says moving our thinking away from anecdote-driven decision-making to data-driven decision-making is a real challenge for clinicians.
Professor Patel says the future starts now, but it requires a change of thinking across the profession.
“It is important this data driven approach to medicine is integral to the training of this current generation of doctors and healthcare professionals otherwise we’re not going to get the cultural change down the track.”
The Australian Financial Review