Is the reason behind migrant success related to them leaving their families behind?
New Yorker – Body Scanning

New Yorker: Arrival Rorschach

New Yorker: Male Brain Development
New Yorker: We are being controlled by the random outcomes of a complex system

New Yorker: Schrodinger’s Vet
About your cat, Mr Schrodinger – I have good new and bad news
Yeats: Education is not the filling of a pail, but the lighting of a fire
Healthcare Fraud – the $272 billion swindle
Health-care fraud
The $272 billion swindle
Why thieves love America’s health-care system
INVESTIGATORS in New York were looking for health-care fraud hot-spots. Agents suggested Oceana, a cluster of luxury condos in Brighton Beach. The 865-unit complex had a garage full of Porsches and Aston Martins—and 500 residents claiming Medicaid, which is meant for the poor and disabled. Though many claims had been filed legitimately, some looked iffy. Last August six residents were charged. Within weeks another 150 had stopped claiming assistance, says Robert Byrnes, one of the investigators.
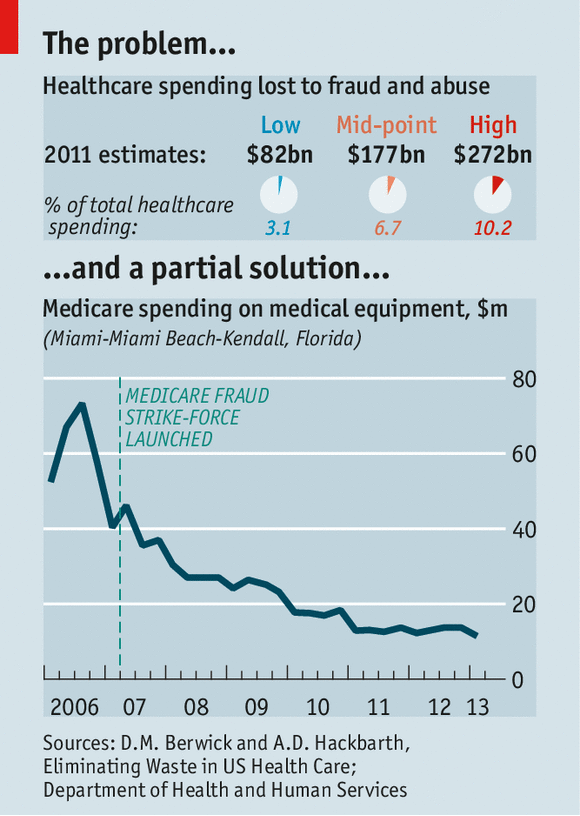
Health care is a tempting target for thieves. Medicaid doles out $415 billion a year; Medicare (a federal scheme for the elderly), nearly $600 billion. Total health spending in America is a massive $2.7 trillion, or 17% of GDP. No one knows for sure how much of that is embezzled, but in 2012 Donald Berwick, a former head of the Centres for Medicare and Medicaid Services (CMS), and Andrew Hackbarth of the RAND Corporation, estimated that fraud (and the extra rules and inspections required to fight it) added as much as $98 billion, or roughly 10%, to annual Medicare and Medicaid spending—and up to $272 billion across the entire health system.
Federal prosecutors had over 2,000 health-fraud probes open at the end of 2013. A Medicare “strike force”, which was formed in 2007, boasts of seven nationwide “takedowns”. In the latest, on May 13th, 90 people, including 16 doctors, were rounded up in six cities—more than half of them in Miami, the capital city of medical fraud. One doctor is alleged to have fraudulently charged for $24m of kit, including 1,000 power wheelchairs.
Punishments have grown tougher: last year the owner of a mental-health clinic got 30 years for false billing. Efforts to claw back stolen cash are highly cost-effective: in 2011-13 the government’s main fraud-control programme, run jointly by the Department of Health and Human Services (HHS) and the Department of Justice, recovered $8 for every $1 it spent.
As fraud-fighting has intensified, dodgy billing has tumbled in areas that were most prone to abuse, such as durable medical kit and home visits (see chart). Home-health fraud—such as charging for non-existent visits to give insulin injections—got so bad that the CMS, which runs the programmes, called a moratorium on enrolling new providers in several large cities last year. Since tighter screening was introduced under Obamacare, the CMS has stripped 17,000 providers of their licence to bill Medicare. Thousands of suppliers also quit after being required to seek accreditation and to post surety bonds of $50,000.
Yet the sheer volume of transactions makes it easier for miscreants to hide: every day, for instance, Medicare’s contractors process 4.5m claims. In this context the $4.3 billion recovered by fraud-busters in 2013, though a record, looks paltry.
Better than cocaine
Fraud migrates. Take one popular scam: overbilling for HIV infusion, an outdated therapy that Medicare still covers despite the existence of cheaper, better alternatives. This scam waned in Florida after a crackdown, only to pop up in Detroit, run by relatives of the original perpetrators.
Fraud mutates, too. As old hustles are rumbled, fraudsters invent new ones. “We’ve taken out much of the low-hanging fruit,” says Gary Cantrell, an investigator at HHS—an example being the thousands of bogus equipment suppliers registered to empty shopfronts. Scams now need to be more sophisticated to succeed, he argues. Doctors, pharmacies, and patients act in league. Scammers over-bill for real services rather than charging for non-existent ones. That makes them harder to spot.
Some criminals are switching from cocaine trafficking to prescription-drug fraud because the risk-adjusted rewards are higher: the money is still good, the work safer and the penalties lighter. Medicare gumshoes in Florida regularly find stockpiles of weapons when making arrests. The gangs are often bound by ethnic ties: Russians in New York, Cubans in Miami, Nigerians in Houston and so on.
Stealing patients’ identities is lucrative. Medical records are worth more to crooks than credit-card numbers. They contain more information, and can be used to obtain prescriptions for controlled drugs. Usually, it takes victims longer to notice that their details have been pinched. The Government Accountability Office has recommended that the CMS remove Social Security numbers from Medicare cards to prevent fraud. It has yet to do so.
In one fast-growing area of fraud, involving pharmacies and prescription drugs, federal investigators have seen caseloads quadruple over the past five years. Elderly patients may receive kickbacks to sell their details to a pharmacist. He will then provide them with drugs they need while billing Medicare for costlier ones.
Paid recruiters scour nursing homes for accomplices. Some pharmacies also pay wholesalers to produce phoney invoices. Others bribe medical workers for leftover pills: in April a pharmacy-owner in Louisiana admitted to paying nursing-home staff a few hundred dollars a time to bring her unused drugs, which she repackaged and sold as new, billing Medicare $2.2m for the recycled meds between 2008 and 2013.
Another scam is to turn a doctor’s clinic into a prescription-writing factory for painkillers (or “pill mill”) and resell them on the street. A clinic in New York was recently charged with fraudulently producing prescriptions for more than 5m oxycodone tablets, which were sold locally for $30-$90 each. The alleged conspirators included doctors and traffickers who ran crews of “patients” so large that long queues sometimes formed outside the clinic. The doctors charged $300 per large prescription. One raked in $12m. To cover their backs they would ask for scans or urine samples purporting to show injuries. The fake patients typically obtained these from the traffickers at the clinic door.
False billing by pharmacies is rife. New York’s Medicaid sleuths have stepped up spot checks to see if the drugs in the back room square with invoices. But this is a lot of work, so most outlets are never checked.
Dozens of operators of ambulances and ambulettes (vans designed to take wheelchairs) have been caught offering kickbacks to patients to pretend they can’t walk. This lets them qualify for “emergency” pick-ups, for which the company can charge $400 per patient. New York has clamped down with roadside checks. But in one case, word that a checkpoint had been set up spread so quickly—as drivers called each other and a local Russian-language radio station put out a warning—that the number of ambulettes on the main street “went from several to none in a few minutes as they re-routed down side streets”, says Chris Bedell, who took part.
This sort of pavement-pounding investigative work remains important. Another approach is the “desk audit”, where possible overpayment is identified but the only way to ascertain losses is to sift through heaps of records manually. Florida’s Agency for Health Care Administration (AHCA) has recovered up to $50m a year solely from hospitals billing for treatment of illegal aliens that is wrongly coded as “emergency care”. But the work is labour-intensive. Data-crunching technologies are increasingly being used to complement the human eye. “When I started in 1996 we had little access to data,” says HHS’s Mr Cantrell. “It had to be requested ad hoc from CMS contractors.” Now a central database houses near-real-time information for Medicare. This helps the 300 workers at the inspector-general’s office who are trained in data analytics to “triage” the tips that flow in. “We receive far more than we can investigate closely,” says Mr Cantrell.
The CMS is still getting to grips with a new predictive-analysis system, which was introduced in 2011 to catch Medicare fraud earlier and is modelled on tools used by credit-card firms. This identified $115m of dodgy payments in 2012, its first full year. (The number for the second year has yet to be released.) Another useful tool is voice-recognition technology. In Florida, health workers who conduct home visits have to call in from the patient’s phone during each appointment to have their voice pattern matched against the one stored electronically. This has greatly reduced billing for non-visits.
Technology is no panacea, however. Medicare’s computers were pumping out thousands of payments a year for patients who had been struck off the programme before receiving their treatment, until human hands began to intervene this year. The electronification of patient records can allow “cloning”, in which treatments automatically trigger excessive billing codes by defaulting to set templates.
This is the medical world’s “dirty secret”, says John Holcomb of the Texas Medical Association. Everyone talks about it in the doctor’s lounge, but few complain. (What doctors do complain about is the complexity of the bill-coding system: see article.) Moreover, there are gaps in the data picture—some of which could grow. Federal investigators complain that there is no proper national repository for Medicaid information, which is held state-by-state.
A bigger worry is that, as ever more Medicare and Medicaid beneficiaries move to “managed care” (privately administered) plans, government sleuths will have access to less data. This could lead to lower fraud-related recoveries.
Efforts have been made to improve information-sharing between government and private insurers, including the creation of a public-private forum, the National Health Care Anti-Fraud Association (NHCAA). But some insurers are reluctant to take part, fearing that being too open with their data would invite lawsuits over privacy. Fraudsters bank on public and private payers not working together to connect the dots, said Louis Saccoccio, the head of the NHCAA, at a recent hearing.
The NCHAA is pushing for federal immunity guarantees for insurers that share fraud-related information. On May 20th a bipartisan group of senators introduced a bill to make it easier for insurers to share data with Medicare. It would also require Medicare to check new providers for links to firms that have previously swindled the taxpayer (which you might have thought it was already doing).
Obamacare has had a big impact, says Shantanu Agrawal of the CMS. One thing it requires is that when a state kicks out a dodgy Medicaid provider, it shares that information with Medicare, and vice versa. Previously there were legal impediments to doing this, for some reason.
Resources are tight for investigators. New York has a Medicaid investigations division of 110 souls (including support staff) to scrutinise $55 billion of annual payments and 137,000 providers. Gloria Jarmon, an auditor with the HHS, told a recent hearing that budget cuts will probably force it to cut its oversight of Medicare and Medicaid by 20% in this fiscal year. “Everyone [in Congress] is excited that we bring in eight times more than we cost, but that hasn’t translated into more funding,” laments Mr Cantrell.
This squeeze makes it all the more important to enlist help. More than 5,000 old folk have joined “Medicare patrols”, which hold local meetings to raise awareness of common scams. A crucial part of the anti-fraud effort is the new, simpler Explanation of Benefits (summary statement) that lets recipients see who has billed the programme with their identification numbers. This is “a landmark change”, a CMS executive told Congress last year, adding: “Our best weapon in fighting fraud is our 50m Medicare beneficiaries.”
http://www.economist.com/news/united-states/21603078-why-thieves-love-americas-health-care-system-272-billion-swindle
Medicity: Entering a new era of population health
Payers are primary drivers toward PHM, and the Centers for Medicare & Medicaid Services is accelerating its timeline for shifting Medicare to a value-based system. By the end of 2016, at least 30 percent of fee-for-service Medicare payments will be tied to value through alternative payment models such as accountable care organizations or bundled payment arrangements. By the end of 2018, that will increase to 50 percent.
http://www.healthcareitnews.com/news/entering-new-era-population-health?single-page=true
Brian Ahier is the director of standards and government affairs at Medicity.
Entering a new era of population health
We have reached an inflection point in the history of health IT
February 18, 2015
In the six years since it became law, the HITECH Act has done much to advance the use of health information technology. And although the process of collecting and sharing health data has not yet significantly impacted care costs or quality, it has laid an important foundation for us to move toward population health management.
[See also: Population health success depends on good data]
There are important discussions underway to determine what’s needed to leverage health data to improve clinicaloutcomes and lower costs, and to extend those benefits across entire patient populations. Intelligent tools for population health will enable improvements in care quality, clinical outcomes and care cost.
Working through issues around health data exchange and patient engagement indicate the next challenges. We must construct a platform that will enable innovation in population health and analytics to thrive.
[See also: Pop health analytics top ACO priority]
Federal entities responsible for overseeing health and the healthcare industry in general are advancing rapidly toward a vision of interoperability and data sharing.
 Congress taking a look
Congress taking a look
Congress is taking both near- and long-term actions regarding health IT innovation and standards. Near-term examples include recently directing the Office of the National Coordinator to report progress around interoperability and data sharing, and asking the Government Accountability Office to report on health information exchanges.
Congress has also launched the “21st Century Cures” initiative to help laws keep pace with health innovation. Among other measures, this initiative would consolidate meaningful use, quality reporting and value-based payments into one program – potentially the most significant move related to population health by Congress to date.
Federal Health IT Strategic Plan and Interoperability Roadmap
This past December, the Department of Health and Human Services released the Federal Health IT Strategic Plan, a coordinated effort among more than 35 federal departments and agencies to advance the collection, sharing and use of electronic health information – the cornerstones of population health management.
The HHS plan’s data-sharing section references the ONC’s Connecting Health and Care for the Nation: A Shared Nationwide Interoperability Roadmap Version 1.0, which was released at the end of January. The roadmap advances the ambitious goals to be reached by the end of 2017, including:
- Establishing a coordinated governance framework and process for nationwide health IT interoperability;
- Improving technical standards and implementation guidance for sharing and using a common clinical data set;
- Enhancing incentives for sharing electronic health information according to common technical standards; and
- Clarifying privacy and security requirements that enable interoperability.
In announcing the roadmap, HHS Secretary Sylvia Burwell called for “an interoperable health IT system where information can be collected, shared and used to improve health, facilitate research and inform clinical outcomes. This Roadmap explains what we can do over the next three years to get there.”
 ONC Annual Meeting
ONC Annual Meeting
At the February 2015 ONC Annual Meeting, titled “Interoperable Health IT for a Healthy Nation,” National Coordinator Karen DeSalvo, MD, told attendees that the agency’s focus is moving beyond meaningful use, toward interoperability and outcomes. This includes building out the IT infrastructure that will support health reform and enable better population health management.
A highlight of the ONC Annual Meeting was having all of the former national coordinators talk about the national state of health IT in the past, present and future.
David Brailer, MD, the nation’s first national coordinator, said the industry won’t be able to accomplish appropriate risk management, population health management or payment reform without interoperability. The ONC leaders shared a strong consensus that the intelligent use of technology will prevail in realizing population health goals.
Meaningful use is not dead
Despite the notion that it may be time to move beyond meaningful use, the program continues to drive electronic health record adoption, organizations have built incentive payments into their IT budgets and we continue to see program improvements.
At the time of this writing, proposed rules for Stage 3 meaningful user and 2015 Edition Standards and Certification Criteria were at the Office of Management and Budget for final review. The OMB announced of the proposed rules that “Stage 3 will focus on improving health care outcomes and further advance interoperability.” Additional recent policy adjustments instituted or proposed include:
- Simplifying satisfaction of the requirement for summary of care transmissions;
- More realistic measures around the availability and actual viewing of patient information to satisfy patient engagement requirements; and
- A potential new requirement to send electronic notification of significant patient health care events to patient care teams.
Measures such as these point to the importance of data sharing and enable achievable and meaningful progress toward population health management.
Payment models increasingly emphasize population health
Payers are primary drivers toward PHM, and the Centers for Medicare & Medicaid Services is accelerating its timeline for shifting Medicare to a value-based system. By the end of 2016, at least 30 percent of fee-for-service Medicare payments will be tied to value through alternative payment models such as accountable care organizations or bundled payment arrangements. By the end of 2018, that will increase to 50 percent.
As recently as 2011, Medicare made almost no payments through alternative payment models.
Among private payers, a group of major providers and insurers have formed the Health Care Transformation Task Force to shift 75 percent of operations to contracts designed to improve quality and lower costs by 2020. These very important public and private payer initiatives strongly underscore the need for critical health IT enablers of effective PHM.
Welcome to the new PHM era of health IT
We have reached an inflection point in the history of health IT, as we move beyond the HITECH era into this new era. We have come a long way in capturing health data, yet have only begun to share that data among providers, patients and payers. The opportunity ahead of us is to take major strides toward using that data to improve care and lower costs for the populace in general. We have been through an incredible decade of health IT. There is no sign of it slowing down.
Topics: Accountable Care, Analytics, Financial/Revenue Cycle Management, Population Health, Quality and Safety,Health Information Technology for Economic and Clinical Health (HITECH) Act, Clinical, Patient Engagement,Interoperability, Meaningful use, Department of Health & Human Services (HHS), The Office of the National Coordinator for Health Information Technology (ONC), Karen DeSalvo, Brailer, David, Electronic Health Record (EHR)
Peter Hinssen: The Tiger and The Rock
EDxBrussels – Peter Hinssen – The TIGER & the ROCK
Why Extrapolating WON’T WORK & What it means for HEALTH http://www.tedxbrussels.eu About TEDx, x = independently organized event In the spirit of ideas worth…
http://wn.com/tedxbrussels_-_peter_hinssen_-_the_tiger_&_the_rock
8:20 – The Contiguous United States – macdonald’s proximity to people in the US
9:10 The Flip: Pharma moving to Health as a Service (no longer a product)
Institutions > Communities (trust)
Reactive > Proactive (attitude)
http://www.datapointed.net/visualizations/maps/distance-to-nearest-mcdonalds-sept-2010/
