In a feat of insitutionalised narcissism, physicians conflate their patients interests with their own, when on the face of it, and many around, they are quite poorly aligned.
Creating a value-based health system will go some way to addressing this…
In a feat of insitutionalised narcissism, physicians conflate their patients interests with their own, when on the face of it, and many around, they are quite poorly aligned.
Creating a value-based health system will go some way to addressing this…
From: http://aushealthit.blogspot.sg/2014/06/senate-estimates-hearing-june-3-2014-e.html
The modus operandi of ‘good’ occupational sociopaths is to convince everyone that all is well, “trust us we know what we are doing”.
The underlying goal is to create as much havoc and confusion as possible, to frustrate, undermine and destroy, whilst on the surface all the while going about their business in a way that looks like we all think they know what the are doing.
Quod erat demonstrandum
Great insights into where capital is being invested in US healthcare…
http://www.healthleadersmedia.com/print/LED-305089/The-Hospital-of-the-Future-is-Not-a-Hospital
I’ve spent a good deal of time the past several weeks interviewing senior healthcare leaders for my story in the May issue of HealthLeaders magazine about the hospital of the future. But in truth, that headline might be a bit of a tease.
As it turns out, the hospital of the future doesn’t look much like a hospital at all. Instead, it’s a cohesive amalgamation of plenty of outpatient modalities that represent growth in healthcare. Inpatient care, increasingly, represents stagnation and shrinkage, in the business sense.
In the past, a story about the hospital of the future has meant investigating healthcare organizations’ access to capital, and their ability to fund expensive new patient bed towers with all-private rooms and top technologies, in a race to grab volume from competitors.
Under that operating scenario, the sky was the limit, in terms of what organizations were willing to do to attract volume.
That calculus has changed drastically.
In a recent survey on healthcare design trends conducted by Minneapolis-based Mortenson Construction, 95% of the healthcare organizations surveyed said most of the projects they are undertaking are predominantly ambulatory in nature.
“If, in theory, the [Patient Protection and Affordable Care Act] has now got 7 million people engaged in healthcare insurance who didn’t have that previously, the inrush of patients will be outpatient-based,” says Larry Arndt, general manager of healthcare in the company’s Chicago offices. “What’s not needed is bed space or heavy procedural space.”
A Strategic Dead End
The PPACA, employers, and commercial health plans have made clear that pursuing expensive inpatient volume in the traditional sense is a strategic dead end. That doesn’t mean new patient towers won’t go up, but it does mean their construction will be based on adaptability, patient flow, and efficiency gains, not bed count.
As few as five to seven years ago, says Arndt, a healthcare leadership team would take a capital improvement project through a planning and programming phase in which they followed a traditional approach. The team would utilize widely standardized metrics and program their building based on what they’re doing now, with no consideration of the future, Arndt says.
By contrast, within the last five years, more leaders have been embracing the concept of lean operational improvement.
In order to be competitive in a limited amount of reimbursements, they have had to become more efficient. So instead of the traditional approach of programming new construction based on how the organization operates today, instead, it attempts to map out its current patient flows and discover how to become more efficient. Only then will the team look at how to build around that improved and more efficient model.
Indeed, a whopping 22% of respondents to Mortenson’s February survey said they were “doing nothing” construction-related right now, and only 5% were planning for a traditional replacement hospital.
Instead, a majority said they are focusing new construction on building clinics that can feature just about any outpatient modality except surgery, Arndt says.
Healthcare Shifts to Outside
They’re focusing on combining dialysis, radiology and other treatments that can be provided in one location. And they’re funneling more of their capital budget to items that are outside the realm of new construction, like home health and what Arndt calls e-home healthcare—in other words, technological solutions that help patients access their caregivers outside of any facility.
“Our customer understands that healthcare is moving more toward healthcare outside a facility,” says Arndt. “That means more money is being invested in health information technology. Also, you see more constellation or satellite projects, for example, a small 15,000-20,000 square-foot clinic in a neighborhood. That allows patients to travel a shorter distance to a less congested environment, but yet allows connection to the bigger facility if needed.”
Modular construction is a trend that Arndt sees developing quickly. It’s in the process of designing a clinic for a client that will feature modular walls, to make it more flexible for the changes in care protocols that are assured, but that healthcare’s leaders aren’t sure how will ultimately affect their competitive offerings.
In one clinic, doctors want to be able to meet with patients in groups, for example. Modular walls mean physicians can occasionally meet with groups of patients instead of individually, or vice-versa. Their space is less limiting.
“The clinic can adapt,” says Arndt.
Prefabricating buildings is also gaining steam in healthcare, he says.
“Money is being invested much more wisely than it has been in the past,” he says. “For the design/construction field, we have to be more lean too.”
Part of that lean attitude means offering customers 3-D modeling that starts with design partners, such as the people who will be staffing the building, to optimize work flow.
Adapting Takes Time
“We can prefab things we couldn’t years ago,” he says. An example might be a bathroom “pod” that can be built offsite and installed on site. Full exam rooms can be prepared the same way, and models can be constructed to test care protocols with the team that will be working there.
Arndt’s customers, he says, can be categorized two ways. Either they’re thinking broadly about adapting to the future without knowing exactly what it’s going to bring, or they’re standing idly on the sideline until they understand better how the PPACA and other drastic changes in how healthcare is provided and paid for will affect their bottom lines.
Neither approach is necessarily better than the other, but waiting just puts off the action that needs to be taken. It can be a prudent approach, but even in healthcare, what works can change quickly. Designing, building, and adapting still takes time.
Don’t wait too long.
Philip Betbeze is senior leadership editor with HealthLeaders Media.
It’s already starting to seem a lot like HSG, except less credible…!
http://rockhealth.com/2014/06/digital-health-entrepreneurs-thoughts-healthkit/

This morning, Apple made its much-anticipated move into healthcare with HealthKit (aka, the formerly rumored HealthBook.) With a typically dissonant and ever-growing ecosystem of health apps, devices and data, digital health needs a major player to enter to integrate these products and tools. We’re excited about what the largest company in the world is capable of doing for digital health. Here’s some perspective on what a seasoned digital health entrepreneur had to say about today.
Aaron Rowe
HealthKit is really exciting. Putting all of this information in one place, in a gorgeous app that will reach a ton of people, could do wonders for public health. But it won’t do much good if the on-screen content is designed without input from people who deeply understand health metrics. It looks like Apple or one of its partners made some technical mistakes on a slide that was shown during the big reveal of their new health app.
The slide, which appeared toward the end of the HealthKit segment of today’s WWDC keynote, neatly displays four key metrics for diabetes management: glucose, carbs, walking, and diabetes medication adherence. The numbers and units that Apple used as examples to illustrate their vision don’t make sense. When you measure your glucose with a personal blood sugar meter, it is measured in mg/dL— but the example shown by Apple displayed these numbers in mL/dL. Whoops!
What’s worse, the app screen features an SMS-style message from a particularly photogenic doctor who says, “You’re making great progress with your diet and exercise. Keep it up.” While the graph above this message shows a steady and very unhealthy looking uptrend in the users glucose readings. The current reading shown on the app is 122 “mL/dL”.
“People with a fasting glucose level of 100 to 125 mg/dL have impaired fasting glucose (IFG), or prediabetes,” according to a National Institute of Diabetes and Digestive and Kidney Diseases website. “A level of 126 mg/dL or above, confirmed by repeating the test on another day, means a person has diabetes.
It strikes me as particularly unusual that Apple would make these mistakes, since they are known for their intense attention to detail. Perhaps this kerfuffle happened because none of the folks who were involved with the WWDC keynote know what medical details should look like—is there some disconnect within the group that is building HealthKit? Have the designers who worked on this screen had enough contact with Apple’s partners at the Mayo Clinic or recently hired health experts? Not long ago, the Cupertino-based company onboarded several noninvasive glucose-monitoring experts from the wearable Raman spectrometer company C8 MediSensors and an early employee of Rock Health’s own Sano Intelligence.
I hope HealthKit will help patients understand and react to the results of every common blood test that is done in the home and medical labs–from cholesterol to creatinine. This could be one of the greatest ways in which Apple can make the world a better place. But they may need to sync internally to refine their understanding of these numbers, before they release this potentially lifesaving product into the wild.
Aaron Rowe is a research director at Integrated Plasmonics, a San Francisco startup that has developed a new class of spectrometer and surface plasmon resonance sensor chips. He and his colleagues are exploring ways to expand the scope of chronic disease management programs, enhance the success of new medications, and increase the usefulness of telemedicine by bringing a wide variety of in vitro diagnostics devices into the home and workplace. You can follow him on Twitter at @soychemist
Was watching Philomena on the plane to Singapore surrounded by 2 families each with 3 children under three. Let’s just say I was luck to have remembered my Seinnheisser DJ Headphones that blocked most of the noise out.
Anyway, it struck me that the relationship between children and their parents, orphans and their churches is similar to Stockholm Syndrome… Wikipedia seems all across it:
Stockholm syndrome, or capture-bonding, is a psychological phenomenon in which hostages express empathy and sympathy and have positive feelings toward their captors, sometimes to the point of defending and identifying with them. These feelings are generally considered irrational in light of the danger or risk endured by the victims, who essentially mistake a lack of abuse from their captors for an act of kindness.[1][2] The FBI‘s Hostage Barricade Database System shows that roughly 8% of victims show evidence of Stockholm syndrome.[3]
Stockholm syndrome can be seen as a form of traumatic bonding, which does not necessarily require a hostage scenario, but which describes “strong emotional ties that develop between two persons where one person intermittently harasses, beats, threatens, abuses, or intimidates the other.”[4] One commonly used hypothesis to explain the effect of Stockholm syndrome is based on Freudian theory. It suggests that the bonding is the individual’s response to trauma in becoming a victim. Identifying with the aggressor is one way that the ego defends itself. When a victim believes the same values as the aggressor, they cease to be a threat.[5]
Battered-person syndrome is an example of activating the capture-bonding psychological mechanism, as are military basic training and fraternity bonding byhazing.[dubious ].[6][7][8]
Stockholm syndrome is sometimes erroneously referred to as Helsinki syndrome.[9][10] Helsinki syndrome is more of a case of group think and inattentional blindnessto the negative in order to achieve some perceived benefit, a reference to the non-binding Helsinki Accords that attempted to settle post WWII Cold War tensions.
“Capitalism is the extraordinary belief that the nastiest of men for the nastiest of motives will somehow work for the benefits of all.”
John Maynard Keynes
http://www.theguardian.com/artanddesign/jonathanjonesblog/2014/may/21/bill-viola-matryr-video-installation-st-pauls
http://www.theguardian.com/artanddesign/video/2014/may/21/bill-viola-martyrs-video-st-pauls-cathedral
• Bill Viola’s second coming: watch the eerie video installation Martyrs here

Bill Viola has created a powerful modern altarpiece for St Paul’s Cathedral that perfectly suits the restrained spirituality of this most English of churches.
Coming into Christopher Wren’s great building on a weekday morning when crowded buses surround this London icon, you notice how ascetic its atmosphere is. Greek mosaics and the perfect geometry of a dome that suggests the clockwork universe of Wren’s contemporary Isaac Newton make St Paul’s a place of cool, even philosophical, prayer.
Bloody martyrdoms, harrowing images of saints being crucified upside down or tortured with hot pincers – such gut-wrenching pictures are deliberately sidelined in the temple of reason that is St Paul’s. At least, they were untilAmerican visionary Viola unveiled his latest work, a permanent video installation, there on Tuesday.
It has taken more than a decade to agree on, plan and install Viola’s eerie multiscreen work Martyrs (Earth, Air, Fire, Water), a quest that started when the cathedral’s overseers were struck by his exhibition The Passions at the National Gallery in 2003. This exhibition revealed the depth of his interest in traditional religious art. St Paul’s has a steady programme of commissioning modern works but there simply is no other artist today of Viola’s quality who is so committed to the idea of religious art. He is making a second work for St Paul’s, to be unveiled next year, called Mary. He says he hopes the pieces are not just art but “practical objects of traditional contemplation and devotion”.
Martyrs is a study in suffering and redemption. Four people on four vertical screens undergo extreme fates: one has been buried, another hangs with her wrists and ankles bound, another sits amid flames and a fourth hangs upside down as he is drenched in cascades of water. As these images develop and transform in parallel, it becomes hard to know what is death and what is hope. Soil is whirled off the buried man in an upward band of dust, like the zip in aBarnett Newman painting, until he is born again, looking up into heavenly light. Similarly, the suspended woman endures her pain to raise her eyes to that light in a final deathly pose of triumph.
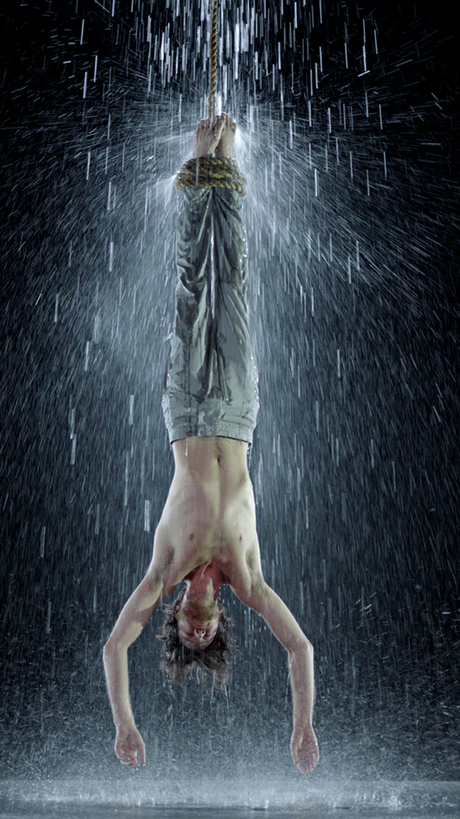 Water … Martyrs by Bill ViolaFrom one point of view, Viola has given the Church of England a visceral shot in the arm, a healthy dose of baroque religious art, a blast of hi-tech Caravaggio. His installation is not literally an altarpiece, but a carbon-steel frame containing four plasma screens that irrestibly evoke medieval polyptych altar paintings. It is subtly situated at the end of an arched aisle with a vista that draws you gradually towards it.
Water … Martyrs by Bill ViolaFrom one point of view, Viola has given the Church of England a visceral shot in the arm, a healthy dose of baroque religious art, a blast of hi-tech Caravaggio. His installation is not literally an altarpiece, but a carbon-steel frame containing four plasma screens that irrestibly evoke medieval polyptych altar paintings. It is subtly situated at the end of an arched aisle with a vista that draws you gradually towards it.
This is no shocking gorefest, despite a sado-masochist suggestiveness that nicely challenges clerical banalities (occasionally looking at these bound bodies I thought of Robert Mapplethorpe‘s photographs). Rather, Viola transforms the idea of martyrdom from some horrific intestine-spilling scene that might terrorise a south Italian church into something eerily still, silent and thought-provoking.
 Earth … Martyrs by Bill ViolaHis martyrs do not scream or bleed or even pray. They silently endure their strange fates. The stress is not on numbing details of torture – the man engulfed by fire is not singed. It is on the mystery of human courage that can endure the impossible. Is such strength god-given? Where then does it come from? Viola gets to the core of what martyrdom means. Through video art, he reframes the philosophical questions it has raised ever since Socrates refused to escape his unjust execution in ancient Athens.
Earth … Martyrs by Bill ViolaHis martyrs do not scream or bleed or even pray. They silently endure their strange fates. The stress is not on numbing details of torture – the man engulfed by fire is not singed. It is on the mystery of human courage that can endure the impossible. Is such strength god-given? Where then does it come from? Viola gets to the core of what martyrdom means. Through video art, he reframes the philosophical questions it has raised ever since Socrates refused to escape his unjust execution in ancient Athens.
Martyrs fits beautifully into the cerebral ambience of St Paul’s because it invites you to contemplate what it is to die for a cause, in much the same intensified yet sombre way one contemplates the mysteries of space and time while looking up into Wren’s Newtonian dome.
Bill Viola is one of the most important artists of our time because he has the bravery to engage with these big questions, and the clarity to do so in a universally compelling way. Atheists have not yet built any special spaces for this kind of deep art, so a church is a fine place to see his work. He takes his spot in St Pauls with becoming modesty and genuine profundity.
so we established yesterday that change on it’s own does not inoculate against tyranny.
but at jen’s urging, I’ve taken the next step to:
stasis is tyranny
{kind=link}