Danebo Elementary in Eugene, Ore., is one of 50 schools receiving money to teach classes while integrating something called the “Good Behavior Game.” Teacher Cami Railey sits at a small table, surrounded by four kids. She’s about to teach them the “s” sound and the “a” sound. But first, as she does every day, she goes over the rules.
“You’re going to earn your stars today by sitting in the learning position,” she says. “That means your bottom is on your seat, backs on the back of your seat. Excellent job, just like that.”
For good learning behavior, like sitting quietly, keeping their eyes on the teacher and working hard, kids get a star and some stickers.
Railey says the game keeps the kids plugged in and therefore learning more. That in turn makes them better educated teens and adults who’re less likely to pick up a dangerous habit, like smoking.
The Washington, D.C., nonprofit Coalition for Evidence Based Policy says it works. It did a studythat found that by age 13, the game had reduced the number of kids who had started to smoke by 26 percent — and reduced the number of kids who had started to take hard drugs by more than half.
The fact that a teacher is playing the Good Behavior Game isn’t unusual. What is unusual is that Trillium is paying for it. Part of the Affordable Care Act involves the federal government giving money to states to figure out new ways to prevent people from getting sick in the first place.
So Trillium is setting aside nearly $900,000 a year for disease prevention strategies, like this one. Jennifer Webster is the disease prevention coordinator for Trillium Community Health, and she thinks it’s a good investment.
“The Good Behavior Game is more than just a game that you play in the classroom. It’s actually been called a behavioral vaccine,” she says. “This is really what needs to be done. What we really need to focus on is prevention.”
Trillium is paying the poorer schools of Eugene’s Bethel School District to adopt the strategy in 50 classrooms.
Trillium CEO Terry Coplin says changes to Oregon and federal law mean that instead of paying for each Medicaid recipient to get treatment, Trillium gets a fixed amount of money for each of its 56,000 Medicaid recipients. That way Trillium can pay for disease prevention efforts that benefit the whole Medicaid population, not just person by person as they need it.
“I think the return on investment for the Good Behavior Game is going to be somewhere in the neighborhood of 10 to one,” Coplin says.
So, for each dollar spent on playing the game, the health agency expects to save $10 by not having to pay to treat these kids later in life for lung cancer because they took up smoking.
Coplin concedes that some of Trillium’s Medicaid recipients will leave the system each year. But he says prevention still makes medical and financial sense.
“All the incentives are really aligned in the right direction. The healthier that we can make the population, the bigger the financial reward,” he says.
The Oregon Health Authority estimates that each pack of cigarettes smoked costs Oregonians about $13 in medical expenses and productivity losses.
Not all the money Trillium is spending goes for the Good Behavior Game. Some of it is earmarked to pay pregnant smokers cold, hard cash to give up the habit. There’s also a plan to have kids try to buy cigarettes at local stores, then give money to store owners who refuse to sell.
This story is part of a reporting partnership with NPR, Oregon Public Broadcasting and Kaiser Health News.
It’s not uncommon for a scientific study to raise more questions than it answers. A fascinating example of this is a study published earlier this month that found that mice can pass a fearful memory down to their offspring — and even the next generation after that. Mice in these later generations froze in fear when they caught a whiff of a certain smell that their fathers (or grandfathers) had learned to associate with an electric shock. Additional experiments showed the same effect when Mom was the one with the scary experience.
The researchers made sure the younger mice had never experienced the smell themselves until it was time to test them, and even mice born through in vitro fertilization who never met their fathers had the fearful memory, seemingly ruling out the possibility that they somehow picked it up from Dad.
The study has spurred an animated debate about how this could happen. The brains of fearful progeny contained more neurons with receptors for the scary smell, the scientists found. They suggest that epigenetic changes — that is, chemical changes to DNA that alter the way genes work — could account for the persistence of memory through the generations. But how such changes could transfer from the brain, where the memory forms, to the sperm and eggs that create the next generation, remains — at least for now — a haunting mystery.
Making organs from stem cells
This year scientists announced several big steps towards engineering functioning organs from stem cells. The colorful blob above is a mini brain created from stem cells derived from reprogrammed human skin cells. By providing just the right chemical environment, European scientists coaxed the stem cells to become neurons and arrange themselves into different structures that crudely resemble the anatomy of a developing fetal brain. The researchers are using these methods to study what goes wrong in developmental brain disorders like microcephaly, using stem cells from individual patients.
Meanwhile, researchers in Japan developed functional human liver tissue from reprogrammed skin cells and several teams reported progress on developing kidney tissue. The road to creating transplantable tissues from stem cells is still long, but these are encouraging steps.
Image: Madeline A. Lancaster
Implantable electronics
Forget wearable electronics — 2013 was a banner year for electronics designed to work from inside the body. Scientists developed biodegradable circuits that could one day destroy microbes with heat to help heal a wound and dissolve after they’ve done their jobs. They invented flexible electronic tattoosthat could be loaded with enough sensors to make your FitBit seem like a clunky piece of junk. And now we have tiny LED probes and a stretchy foil made of gold nanoparticles that can measure and manipulate the brain. Your cyborg future just got a little closer.
This hour long presentation covers the key points from Taleb’s Antifragile. It doesn’t matter how often I read or listen to this, it still comes across as massive. Interesting that the UK conservatives are taking it up with vigor, hmm….
In 2006 Nassim Taleb came to prominence with the publication of The Black Swanand the idea that the world is full of highly improbably and unpredictable events. In his latest book Antifragile he explains how to live with, and respond to, these seemingly random and unforeseen black swan events.
The key he says is to create systems that are Antifragile; ones that are not simply robust or resilient but can adapt and improve when subjected to uncertainty, chaos and volatility.
Highlights of Antifragile – RSA (UK) 6th Dec. 2012
Distinguished Professor of Risk Engineering at New York University’s Polytechnic Institute.
Author of ‘Antifragile: how to live in a world we don’t understand’ (Allen Lane, 2012).
Rohan Silva
Senior policy adviser to UK Prime Minister, David Cameron.
The latest fitness trend in offices around the country is employees giving up their chairs in order to stand while working. Now Stir, a Pasadena, CA company, is helping this fitness cause with their smart desk called Stir Kinetic that adapts to the user’s position and also helps track the additional calories burned due to standing.
In order to start using the Stir Kinetic desk, the user has to first enter his or her standing and sitting heights, as well as the amount of time he or she would like to stand per day while working, using the touch screen console on the desk surface. The hardwood desk then uses motors to move its position from seated height to standing height by a mere double tap on the console. The smart desk tracks the amount of standing time per day in order to provide the user a count of the calories burned and has a Whisperbreath feature that automatically changes the desk’s height by one inch up or down, forcing the user to change positions, thereby incorporating some physical activity into office jobs.
The algorithm running the Stir Desk works to create changes in desk height at appropriate times and tracks the user’s work patterns to teach itself the best times to coax the user to change positions. The smart desk has been equipped with Bluetooth and WiFi connectivity to be able to transmit data to a smartphone in the future and Stir aims to roll out wellness and fitness smartphone apps that work with the smart desk.
The desk is currently available for purchase for a premium price of $3890, and comes in two top surface color options of either white lacquer or espresso-stained.
The Asymptotic Shift From Disease To Prevention–Thoughts For Digital Health
It’s been said that good artists borrow and great artist steal. And I believe that Picasso was right. So, I guess I’m somewhere between a thief and a artist and that suits me just fine.
I’ve stolen from two great thinkers, so let’s get that out of the way. The first isDaniel Kraft, MD. Daniel Kraft is a Stanford and Harvard trained physician-scientist, inventor, entrepreneur, and innovator. He’s the founded and Executive Director of FutureMed, a program that explores convergent, rapidly developing technologies and their potential in biomedicine and healthcare. He’s also a go-to source on digital health. I’m stealing “zero stage disease” from Dr. Kraft. Simply put, it’s the concept of disease at its most early, sub-clinical stage. It’s a point where interventions can halt or change a process and potentially eliminate any significant manifestation of disease.
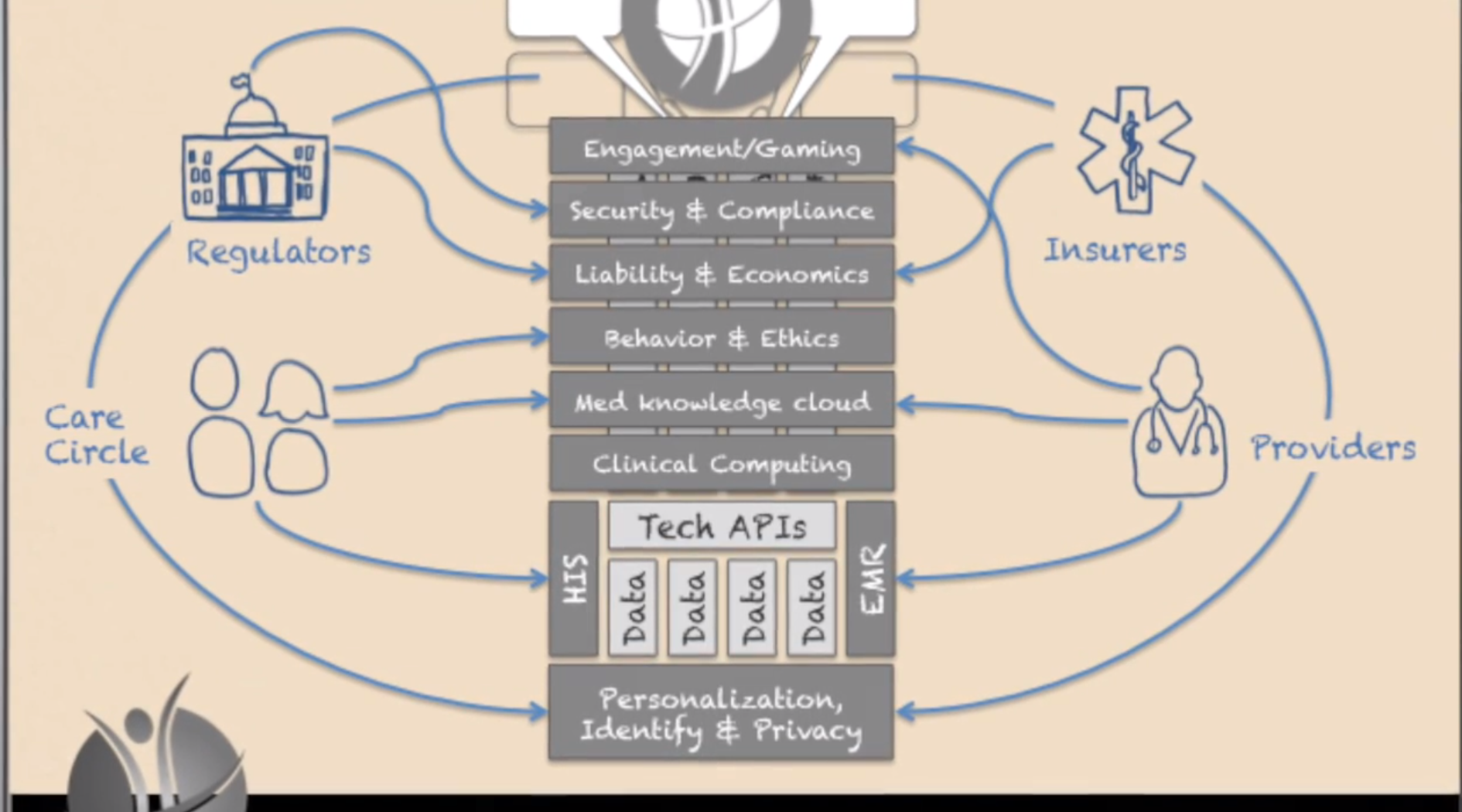
The second source of inspiration is Richie Etwaru. He is a brilliant and compelling speaker and a champion for global innovation, Mr. Etwaru, is responsible for defining and delivering the global next generation enterprise product suite for health and life sciences at Cegedim RelationshipManagement. His inspiring video, The Future of Human API really got me thinking.
At the heart of Mr. Etwaru’s discussion is the emergence of prevention–not treatment–as the “next big thing”.
Ok, nothing new so far. But the important changes seen in the digital health movement have given us a profound opportunity to move away from the conventional clinical identification of a that golf-ball sized tumor in your chest to a much more sophisticated and subtle observation. We are beginning to find a new disease stage–different from the numbers and letters seen in cancer staging. The disease stage is getting closer and closer to zero. It’s taking an asymptotic path that connects disease with prevention. The point here is that the holy grail of prevention isn’t born of health and wellness. Prevention is born out of disease and our new-found ability to find it by looking closer and earlier. Think quantified self and Google Calico.
And here lies the magic.
We all live in the era of disease. And the vast majority of healthcare costs are spent after something happens. The simple reality is that prevention is difficult to fund and the health-economic model is so skewed to sickness and the end of life that it’s almost impossible to change. But if we can treat illness earlier and earlier–the concept of an asymptote–we build a model where prevention and disease share the very same border. They become, in essence, the same. And it’s here that early, early, early disease stage recognition (Stage Zero) becomes prevention. The combination of passive (sensor mediated) observation and proactive life-style strategies for disease suppression can define a new era of health and wellness.
Keep Critical! Follow me on Twitter and stay healthy!
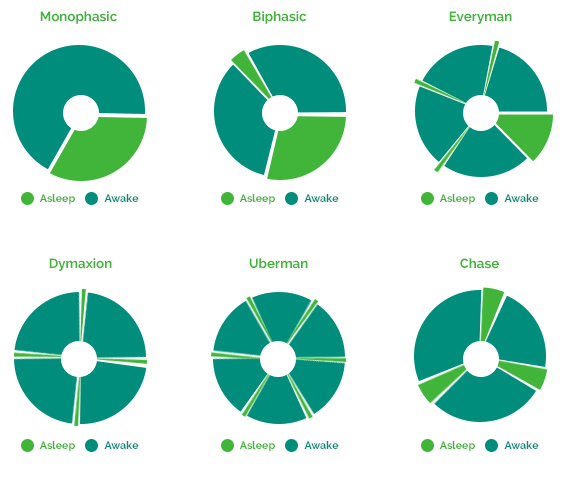
It is a term referring to alternate sleep patterns that can reduce the required sleep time to just 2-6 hours daily. It involves breaking up your sleep into smaller parts throughout the day, which allows you to sleep less but feel as refreshed as if you slept for 8 hours or more.
Polyphasic sleep modes
Simply put, it’s a series of fine-tuned power naps that allow you to sleep effectively, rest better and perform at optimum energy levels during the day.
Additionally, NeuroOn monitored polyphasic sleep allows you to sync your body clock to very demanding schedules at whatever time is convenient or required.
In conclusion, through great sleep efficiency, Polyphasic sleep can give you an extra 4 hours of free time every day. That’s up to 28 hours (1 day+) a week, 1460 hours a year.
That’s right – Your year now has over 420 working days!
Trust the masters
So, you’ve heard of Leonardo? No, not the turtle!
Apparently Da Vinci, Tesla, Churchill and even Napoleon used polyphasic sleep to rest. It allowed them to fully regenerate, reducing sleep time to 6.5 hours or sometimes just 2 hours. And those guys got things done!
Right. So I’m now comfortable with the idea that the greatest failing of modern healthcare is for it to have extended lifespan without having extended healthy life years. The challenge then, is to extend fully productive life to something far closer to our life expectancy. This can be done with a plant based diet, fasting and moderate exercise. No pills. No fads. Jus a new norm.
But how do we pay for it? Determine the economic cost of extending a life’s productivity by a year seems like a reasonable first step. Then take a piece of that?
Bring in the direct beneficiaries of such a change – the life insurers, super funds and broccoli farmers.
What a great bunch of business partners they’d be.
Top piece on Sinai’s vision. Everything’s lined up there except the doctors – hmmm…. They’ll need some amazing insights to bust through the inertia, but expect they’ll glean them…
In The Hospital Of The Future, Big Data Is One Of Your Doctors
December 5, 2013 | 7:30 AM
From our genomes to Jawbones, the amount of data about health is exploding. Bringing on top Silicon Valley talent, one NYC hospital is preparing for a future where it can analyze and predict its patients’ health needs–and maybe change our understanding of disease.
The office of Jeff Hammerbacher at Mount Sinai’s Icahn School of Medicine sits in the middle of one of the most stark economic divides in the nation. To Hammerbacher’s south are New York City’s posh Upper East Side townhouses. To the north, the barrios of East Harlem.
What’s below is most interesting: Minerva, a humming supercomputer installed last year that’s named after the Roman goddess of wisdom and medicine.
It’s rare to find a supercomputer in a hospital, even a major research center and medical school like Mount Sinai. But it’s also rare to find people like Hammerbacher, a sort of human supercomputer who is best known for launching Facebook’s data science teamand, later, co-founding Cloudera, a top Silicon Valley “big data” software company where he is chief scientist today. After moving to New York this year to dive into a new role as a researcher at Sinai’s medical school, he is setting up a second powerful computing cluster based on Cloudera’s software (it’s called Demeter) and building tools to better store, process, mine, and build data models. “They generate a pretty good amount of data,” he says of the hospital’s existing electronic medical record system and its data warehouse that stored 300 million new “events” last year. “But I would say they are only scratching the surface.”
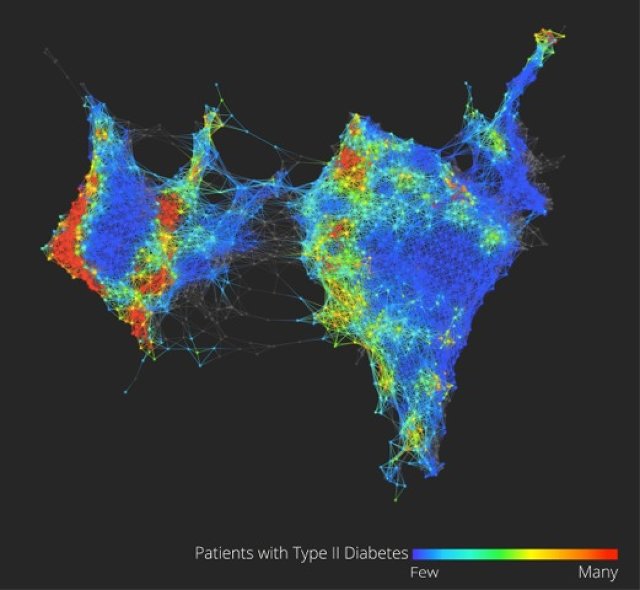
Could there actually be three types of Type 2 diabetes? A look at the health data of 30,000 volunteers hints that we know less than we realize. Credit: Li Li, Mount Sinai Icahn School of Medicine, and Ayasdi
Combined, the circumstances make for one of the most interesting experiments happening in hospitals right now–one that gives a peek into the future of health care in a world where the amount of data about our own health, from our genomes to ourJawbone tracking devices, is exploding.
“What we’re trying to build is a learning health care system,” says Joel Dudley, director of biomedical informatics for the medical school. “We first need to collect the data on a large population of people and connect that to outcomes.”
To imagine what the hospital of the future could look like at Mount Sinai, picture how companies like Netflix and Amazon and even Facebook work today. These companies gather data about their users, and then run that data through predictive models and recommendation systems they’ve developed–usually taking into account a person’s past history, maybe his or her history in other places on the web, and the history of “similar” users–to make a best guess about the future–to suggest what a person wants to buy or see, or what advertisement might entice them.
Through real-time data mining on a large scale–on massive computers like Minerva–hospitals could eventually operate in similar ways, both to improve health outcomes for individual patients who enter Mount Sinai’s doors as well as to make new discoveries about how to diagnose, treat, and prevent diseases at a broader, public health scale. “It’s almost like the Hadron Collider approach,” Dudley says. “Let’s throw in everything we think we know about biology and let’s just look at the raw measurements of how these things are moving within a large population. Eventually the data will tell us how biology is wired up.”
Dudley glances at his screen to show the very early inklings of this vision of what “big data” brought to the world of health care and medical research could mean.
On it (see the figure above) is a visualization of the health data of 30,000 Sinai patients who have volunteered to share their information with researchers. He points out, in color, three separate clusters of the people who have Type 2 diabetes. What we’re looking at could be an entirely new notion of a highly scrutinized disease. “Why this is interesting is we could really be looking at Type 2, Type 3, and Type 4 diabetes,” says Dudley. “Right now, we have very coarse definitions of disease which are not very data-driven.” (Patients on the map are grouped by how closely related their health data is, based on clinical readings like blood sugar and cholesterol.)
From this map and others like it, Dudley might be able to pinpoint genes that are unique to diabetes patients in the different clusters, giving new ways to understand how our genes and environments are linked to disease, symptoms, and treatments. In another configuration of the map, Dudley shows how racial and ethnic genetic differences may define different patterns of a disease like diabetes–and ultimately, require different treatments.
These are just a handful of small examples of what could be done with more data on patients in one location, combined with the power to process it. In the same way Facebook shows the social network, this data set is the clinical network. (The eventual goal is to enroll 100,000 patients in what’s called the BioMe platform to explore the possibilities in having access to massive amounts of data.) “There’s nothing like that right now–where we have a sort of predictive modeling engine that’s built into a health care system,” Dudley says. “Those methods exist. The technology exists, and why we’re not using that for health care right now is kind of crazy.”
While Sinai’s goal is to use these methods to bring about more personalized diagnoses and treatments for a wide variety of diseases, such as cancer or diabetes, and improve patient care in the hospital, there are basic challenges that need to be overcome in order to making this vision achievable.
Almost every web company was born swimming in easily harvested and mined data about users, but in health care, the struggle has for a long time been more simple: get health records digitized and keep them private, but make them available to individual doctors, insurers, billing departments, and patients when they need them. There’s not even a hospital’s version of a search engine for all its data yet, says Hammerbacher, and in the state the slow-moving world of health care is in today, making predictions that would prevent disease could be just the icing on the cake. “Simply centralizing the data and making it easily available to a broad base of researchers and clinicians will be a powerful tool for developing new models that help us understand and treat disease,” he says.
Sinai is starting to put some of these ideas into clinical practice at the hospital. For example, in a hint of more personalized medicine that could come one day, the FDA is beginning to issue labels for some medicines that dictate different doses for patients who have a specific genetic variant (or perhaps explain that they should avoid the medicine altogether). The “Clipmerge” software that the hospital is beginning to now use makes it easier for doctors to quickly search and be notified of these kinds of potential interactions on an electronic medical record form.
On the prediction side, the hospital has already implemented a predictive model called PACT into its electronic medical record system. It is used to predict the likelihood that a discharged patient will come back to the hospital within 90 days (the new health care law creates financial incentives for hospitals to reduce their 90-day readmission rate). Based on the prediction, a high-risk patient at the medical center now might actually receive different care, such as being assigned post-care coordinator.
Eventually, there will be new kinds of data that can be put in mineable formats and linked to electronic patient records, from patient satisfaction surveys and doctors’ clinical notes to imaging data from MRI scans, Dudley says.
Right now, for example, the growing volumes of data generated from people’s fitness and health trackers is interesting on the surface, but it’s hard to glean anything meaningful for individuals. But when the data from thousands of people are mined for signals and links to health outcomes, Dudley says, it’s likely to prove valuable in understanding new ways to prevent disease or detect it at the earliest signs.
A major limitation to this vision is the hospital’s access to all of these new kinds of data. There are strict federal laws that govern patient privacy, which can make doctors loathe to experiment with ways to gather it or unleash it. And there are many hoops today to transferring patient data from one hospital or doctor to another, let alone from all the fitness trackers floating around. If patients start demanding more control over their own health data and voluntarily provide it to doctors, as Dudley believes patients will start to do, privacy could become a concern in ways people don’t expect or foresee today–just as it has on the Internet.
One thing is clear: As the health care system comes under pressure to cut costs and implement more preventative care, these ideas will become more relevant. Says Dudley: “A lot of people do research on computers, but I think what we’re hoping for is that we’re going to build a health care system where complex models … are firing on an almost day-to-day basis. As patients are getting information about them put in the electronic medical record system there will be this engine in the background.”
This is part of a new series of articles that looks at some of the most bizarre and niche business ideas we see here at Springwise.
Remembering loved ones is a highly personal experience, and placing ashes into an urn can be too traditional for some. The first of our Weird of the Week series focused on Holy Smokes, a service that puts ashes into bullets. Now the UK’s And Vinyly is enabling the recently departed to have their ashes pressed as a vinyl record.
Founded by Jason Leach, who also runs a number of record labels such as Subhead, Daftwerk and Death to Vinyl, the service allows anyone to have a loved one’s ashes pressed as a working record, where it can be accompanied by music, the sound of their voice or simply left blank — allowing the pops and clicks to provide an audio representation of the ashes. The ashes are placed onto the raw piece of vinyl before it gets pressed, enabling the ashes to be compressed into the material. Each record comes with personalized artwork — either a simple name and date of birth and death, or a portrait by artist James Hague, who creates his images using ashes mixed into the paint. The GBP 2,000 package gets customers 30 discs with the sounds of their choice, or they can also have a Daftwerk artist record a song about the deceased.
While some may feel uncomfortable handling the ashes of their loved ones, others may cherish the opportunity to connect with them after they die through a very personal artifact. What other unusual ways are there to commemorate the dead?




 The latest fitness trend in offices around the country is employees giving up their chairs in order to stand while working. Now Stir, a Pasadena, CA company, is helping this fitness cause with their smart desk called Stir Kinetic that adapts to the user’s position and also helps track the additional calories burned due to standing.
The latest fitness trend in offices around the country is employees giving up their chairs in order to stand while working. Now Stir, a Pasadena, CA company, is helping this fitness cause with their smart desk called Stir Kinetic that adapts to the user’s position and also helps track the additional calories burned due to standing.