The Asymptotic Shift From Disease To Prevention–Thoughts For Digital Health
It’s been said that good artists borrow and great artist steal. And I believe that Picasso was right. So, I guess I’m somewhere between a thief and a artist and that suits me just fine.
I’ve stolen from two great thinkers, so let’s get that out of the way. The first isDaniel Kraft, MD. Daniel Kraft is a Stanford and Harvard trained physician-scientist, inventor, entrepreneur, and innovator. He’s the founded and Executive Director of FutureMed, a program that explores convergent, rapidly developing technologies and their potential in biomedicine and healthcare. He’s also a go-to source on digital health. I’m stealing “zero stage disease” from Dr. Kraft. Simply put, it’s the concept of disease at its most early, sub-clinical stage. It’s a point where interventions can halt or change a process and potentially eliminate any significant manifestation of disease.
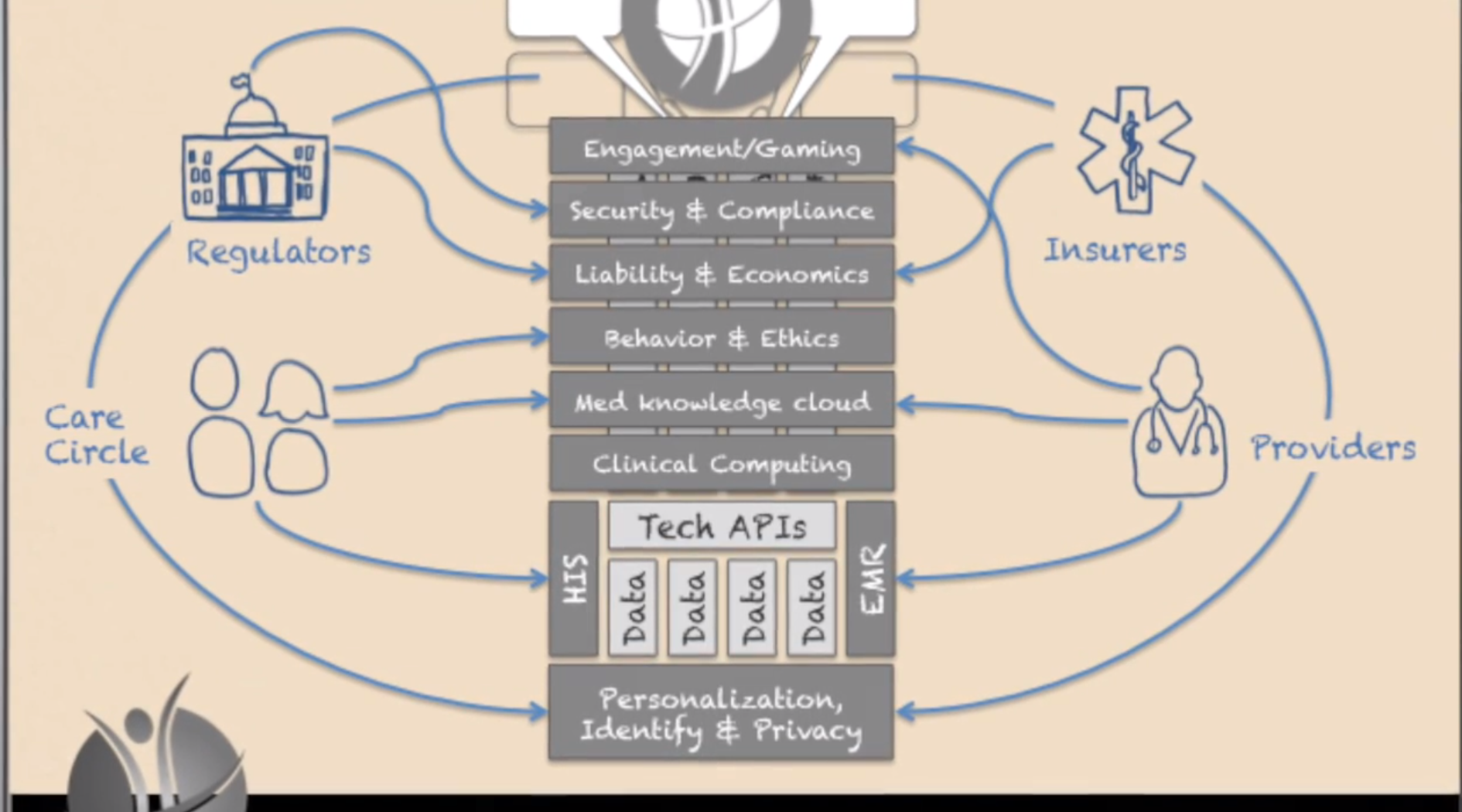
The second source of inspiration is Richie Etwaru. He is a brilliant and compelling speaker and a champion for global innovation, Mr. Etwaru, is responsible for defining and delivering the global next generation enterprise product suite for health and life sciences at Cegedim RelationshipManagement. His inspiring video, The Future of Human API really got me thinking.
At the heart of Mr. Etwaru’s discussion is the emergence of prevention–not treatment–as the “next big thing”.
Ok, nothing new so far. But the important changes seen in the digital health movement have given us a profound opportunity to move away from the conventional clinical identification of a that golf-ball sized tumor in your chest to a much more sophisticated and subtle observation. We are beginning to find a new disease stage–different from the numbers and letters seen in cancer staging. The disease stage is getting closer and closer to zero. It’s taking an asymptotic path that connects disease with prevention. The point here is that the holy grail of prevention isn’t born of health and wellness. Prevention is born out of disease and our new-found ability to find it by looking closer and earlier. Think quantified self and Google Calico.
And here lies the magic.
We all live in the era of disease. And the vast majority of healthcare costs are spent after something happens. The simple reality is that prevention is difficult to fund and the health-economic model is so skewed to sickness and the end of life that it’s almost impossible to change. But if we can treat illness earlier and earlier–the concept of an asymptote–we build a model where prevention and disease share the very same border. They become, in essence, the same. And it’s here that early, early, early disease stage recognition (Stage Zero) becomes prevention. The combination of passive (sensor mediated) observation and proactive life-style strategies for disease suppression can define a new era of health and wellness.
Keep Critical! Follow me on Twitter and stay healthy!
Deborah A. Cohen. A Big Fat Crisis: The Hidden Forces Behind the Obesity Epidemic—And How We Can End It. Nation Books, 2013.
Here’s my blurb:
Deborah Cohen gives us a physician’s view of how to deal with today’s Big Fat Crisis. In today’s “eat more” food environment, Individuals can’t avoid overweight on their own. This extraordinarily well researched book presents a convincing argument for the need to change the food environment to make it easier for every citizen to eat more healthfully.
The conventional wisdom is that overeating is the expression of individual weakness and a lack of self-control. But that would mean that people in this country had more willpower thirty years ago, when the rate of obesity was half of what it is today. Our capacity for self-control has not shrunk; instead, the changing conditions of our modern world have pushed our limits to such an extent that more and more of us are simply no longer up to the challenge.
Right. So I’m now comfortable with the idea that the greatest failing of modern healthcare is for it to have extended lifespan without having extended healthy life years. The challenge then, is to extend fully productive life to something far closer to our life expectancy. This can be done with a plant based diet, fasting and moderate exercise. No pills. No fads. Jus a new norm.
But how do we pay for it? Determine the economic cost of extending a life’s productivity by a year seems like a reasonable first step. Then take a piece of that?
Bring in the direct beneficiaries of such a change – the life insurers, super funds and broccoli farmers.
What a great bunch of business partners they’d be.
Blue Zones employs evidence-based ways to help people live longer, better. The Company’s work is rooted in the New York Times best-selling books TheBlue Zones and Thrive—both published by National Geographic books. In 2009, Blue Zones applied the tenets of the books to Albert Lea, MN and successfully raised life expectancy and lowered health care costs for city workers by 40%. Blue Zones takes a systematic, environmental approach to well-being which focuses on optimizing policy, building design, social networks, and the built environment. The Blue Zones Project is based on this innovative approach.
better diet, exercise, low blood pressure, not smoking and avoiding obesity present key aspects of preventing dementia
Vitamins B6 and B12 and folic acid would cost pennies a day and slowed atrophy of gray matter in brain areas affected by Alzheimer’s disease, according to a study published in May by the Proceedings of the National Academy of Sciences.
Dementia Researchers Call for G-8 to Focus on Prevention
By Andrea Gerlin Dec 10, 2013 9:00 PM ET
The suffering and costs of dementia would be reduced by preventative measures if the Group of Eight nations adopt a model that has worked in fighting heart disease, a group of doctors and scientists said.
“About half of Alzheimer’s disease cases worldwide might be attributable to known risk factors,” they said in a statement before a G-8 meeting in London tomorrow to coordinate responses to the condition. “Taking immediate action on the known risk factors could perhaps prevent up to one-fifth of predicted new cases by 2025.”
The costs of dementia were estimated at $604 billion for 2010, the group said, and the number of cases is set to more than triple by 2050. The 111 signatories from 36 countries called on governments to back more research into prevention, and policies such as promotion of healthier diets. The G-8 are the U.K., U.S., Germany, France, Canada, Italy, Russiaand Japan.
“The choice is stark,” said Zaven Khachaturian, a signatory and editor-in-chief of U.S. journalAlzheimer’s & Dementia. “Either you invest money in creating this infrastructure for preventing or delaying dementia, or continue along the way. If we continue with the current trends, no country’s health-care system will be able to provide care.”
Cheap Vitamins
Alzheimer’s Disease International estimates that 44 million people worldwide have dementia, which will rise to 76 million in 2030 and 135 million by 2050, according to data from the group of Alzheimer’s associations.
About $40 billion has been invested in drug development efforts that haven’t produced effective new medicines, the researchers said in today’s statement. Even so, recent research suggests there may be cheap options to help tackle the problem.
A cocktail of vitamins B6 and B12 and folic acid would cost pennies a day and slowed atrophy of gray matter in brain areas affected by Alzheimer’s disease, according to a study published in May by the Proceedings of the National Academy of Sciences.
About half the fall in deaths from conditions such as heart disease and stroke in the past 50 years resulted from modifying risk factors, according to the scientists advocating prevention. Taking a similar approach to dementia by encouraging middle-aged people to adopt healthy lifestyles may ward off the condition as it does other diseases and save “huge sums,” they said.
Healthy Lifestyle
A healthy lifestyle includes exercising; not smoking; following a diet rich in fruit, vegetables and fish; avoiding obesity, diabetes and excessive alcohol; and treating high blood pressure, the researchers said.
Other research is helping to identify people at risk. A person’s chance of getting dementia before age 65 may develop as early as adolescence, according to a study that suggests teens with high blood pressure or who drink excessively are at risk.
Other risk factors include stroke, use of antipsychotics, father’s dementia, drug intoxication, as well as short stature and low cognitive function, according to the study of Swedish men published by the journal JAMA Internal Medicine in August.
G-8 governments should set goals, stimulate more collaborative research, coordinate policies and establish consistent rules for data sharing, intellectual property and ethics, Khachaturian said in a telephone interview.
The U.S. Food and Drug Administration hasn’t cleared new drugs for memory loss conditions in a decade. Approved medicines such as Eisai Co. (4523)’s Aricept ease symptoms without slowing or curing dementia.
Useful Lessons
A joint U.S.-European Union task force in 2011 found that all disease-modifying treatments for Alzheimer’s in the previous decade failed late-stage trials “despite enormous financial and scientific efforts.” Since then, at least four more experimental treatments have failed.
Eric Karran, director of research at the charity Alzheimer’s Research UK, who wasn’t among the signatories to the statement, said that failed trials can provide useful lessons. One of the four medicines, Eli Lilly & Co. (LLY)’s solanezumab, is undergoing further tests to determine if it helps people with mild Alzheimer’s disease, Karran said.
“If we could just get efficacy in one approach, we will unlock so much else, we will get so much more understanding,” Karran said at a press conference on Dec. 4. “If solanezumab is shown to work in mild Alzheimer’s disease, the pathway will be to take that earlier and earlier.”
Top piece on Sinai’s vision. Everything’s lined up there except the doctors – hmmm…. They’ll need some amazing insights to bust through the inertia, but expect they’ll glean them…
In The Hospital Of The Future, Big Data Is One Of Your Doctors
December 5, 2013 | 7:30 AM
From our genomes to Jawbones, the amount of data about health is exploding. Bringing on top Silicon Valley talent, one NYC hospital is preparing for a future where it can analyze and predict its patients’ health needs–and maybe change our understanding of disease.
The office of Jeff Hammerbacher at Mount Sinai’s Icahn School of Medicine sits in the middle of one of the most stark economic divides in the nation. To Hammerbacher’s south are New York City’s posh Upper East Side townhouses. To the north, the barrios of East Harlem.
What’s below is most interesting: Minerva, a humming supercomputer installed last year that’s named after the Roman goddess of wisdom and medicine.
It’s rare to find a supercomputer in a hospital, even a major research center and medical school like Mount Sinai. But it’s also rare to find people like Hammerbacher, a sort of human supercomputer who is best known for launching Facebook’s data science teamand, later, co-founding Cloudera, a top Silicon Valley “big data” software company where he is chief scientist today. After moving to New York this year to dive into a new role as a researcher at Sinai’s medical school, he is setting up a second powerful computing cluster based on Cloudera’s software (it’s called Demeter) and building tools to better store, process, mine, and build data models. “They generate a pretty good amount of data,” he says of the hospital’s existing electronic medical record system and its data warehouse that stored 300 million new “events” last year. “But I would say they are only scratching the surface.”
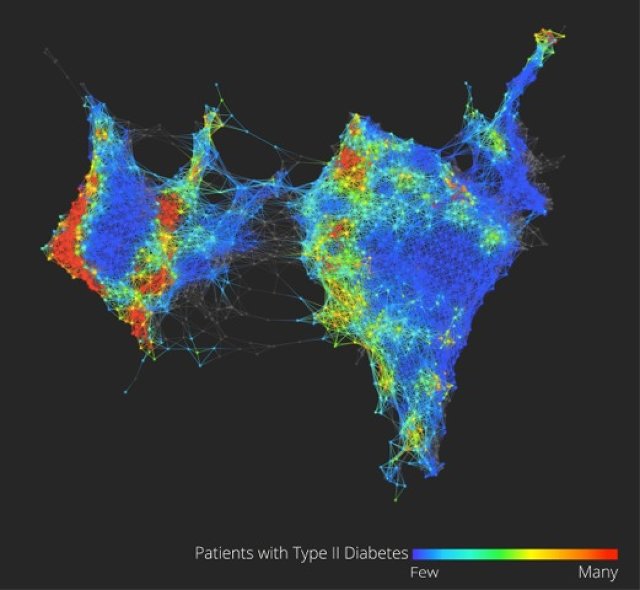
Could there actually be three types of Type 2 diabetes? A look at the health data of 30,000 volunteers hints that we know less than we realize. Credit: Li Li, Mount Sinai Icahn School of Medicine, and Ayasdi
Combined, the circumstances make for one of the most interesting experiments happening in hospitals right now–one that gives a peek into the future of health care in a world where the amount of data about our own health, from our genomes to ourJawbone tracking devices, is exploding.
“What we’re trying to build is a learning health care system,” says Joel Dudley, director of biomedical informatics for the medical school. “We first need to collect the data on a large population of people and connect that to outcomes.”
To imagine what the hospital of the future could look like at Mount Sinai, picture how companies like Netflix and Amazon and even Facebook work today. These companies gather data about their users, and then run that data through predictive models and recommendation systems they’ve developed–usually taking into account a person’s past history, maybe his or her history in other places on the web, and the history of “similar” users–to make a best guess about the future–to suggest what a person wants to buy or see, or what advertisement might entice them.
Through real-time data mining on a large scale–on massive computers like Minerva–hospitals could eventually operate in similar ways, both to improve health outcomes for individual patients who enter Mount Sinai’s doors as well as to make new discoveries about how to diagnose, treat, and prevent diseases at a broader, public health scale. “It’s almost like the Hadron Collider approach,” Dudley says. “Let’s throw in everything we think we know about biology and let’s just look at the raw measurements of how these things are moving within a large population. Eventually the data will tell us how biology is wired up.”
Dudley glances at his screen to show the very early inklings of this vision of what “big data” brought to the world of health care and medical research could mean.
On it (see the figure above) is a visualization of the health data of 30,000 Sinai patients who have volunteered to share their information with researchers. He points out, in color, three separate clusters of the people who have Type 2 diabetes. What we’re looking at could be an entirely new notion of a highly scrutinized disease. “Why this is interesting is we could really be looking at Type 2, Type 3, and Type 4 diabetes,” says Dudley. “Right now, we have very coarse definitions of disease which are not very data-driven.” (Patients on the map are grouped by how closely related their health data is, based on clinical readings like blood sugar and cholesterol.)
From this map and others like it, Dudley might be able to pinpoint genes that are unique to diabetes patients in the different clusters, giving new ways to understand how our genes and environments are linked to disease, symptoms, and treatments. In another configuration of the map, Dudley shows how racial and ethnic genetic differences may define different patterns of a disease like diabetes–and ultimately, require different treatments.
These are just a handful of small examples of what could be done with more data on patients in one location, combined with the power to process it. In the same way Facebook shows the social network, this data set is the clinical network. (The eventual goal is to enroll 100,000 patients in what’s called the BioMe platform to explore the possibilities in having access to massive amounts of data.) “There’s nothing like that right now–where we have a sort of predictive modeling engine that’s built into a health care system,” Dudley says. “Those methods exist. The technology exists, and why we’re not using that for health care right now is kind of crazy.”
While Sinai’s goal is to use these methods to bring about more personalized diagnoses and treatments for a wide variety of diseases, such as cancer or diabetes, and improve patient care in the hospital, there are basic challenges that need to be overcome in order to making this vision achievable.
Almost every web company was born swimming in easily harvested and mined data about users, but in health care, the struggle has for a long time been more simple: get health records digitized and keep them private, but make them available to individual doctors, insurers, billing departments, and patients when they need them. There’s not even a hospital’s version of a search engine for all its data yet, says Hammerbacher, and in the state the slow-moving world of health care is in today, making predictions that would prevent disease could be just the icing on the cake. “Simply centralizing the data and making it easily available to a broad base of researchers and clinicians will be a powerful tool for developing new models that help us understand and treat disease,” he says.
Sinai is starting to put some of these ideas into clinical practice at the hospital. For example, in a hint of more personalized medicine that could come one day, the FDA is beginning to issue labels for some medicines that dictate different doses for patients who have a specific genetic variant (or perhaps explain that they should avoid the medicine altogether). The “Clipmerge” software that the hospital is beginning to now use makes it easier for doctors to quickly search and be notified of these kinds of potential interactions on an electronic medical record form.
On the prediction side, the hospital has already implemented a predictive model called PACT into its electronic medical record system. It is used to predict the likelihood that a discharged patient will come back to the hospital within 90 days (the new health care law creates financial incentives for hospitals to reduce their 90-day readmission rate). Based on the prediction, a high-risk patient at the medical center now might actually receive different care, such as being assigned post-care coordinator.
Eventually, there will be new kinds of data that can be put in mineable formats and linked to electronic patient records, from patient satisfaction surveys and doctors’ clinical notes to imaging data from MRI scans, Dudley says.
Right now, for example, the growing volumes of data generated from people’s fitness and health trackers is interesting on the surface, but it’s hard to glean anything meaningful for individuals. But when the data from thousands of people are mined for signals and links to health outcomes, Dudley says, it’s likely to prove valuable in understanding new ways to prevent disease or detect it at the earliest signs.
A major limitation to this vision is the hospital’s access to all of these new kinds of data. There are strict federal laws that govern patient privacy, which can make doctors loathe to experiment with ways to gather it or unleash it. And there are many hoops today to transferring patient data from one hospital or doctor to another, let alone from all the fitness trackers floating around. If patients start demanding more control over their own health data and voluntarily provide it to doctors, as Dudley believes patients will start to do, privacy could become a concern in ways people don’t expect or foresee today–just as it has on the Internet.
One thing is clear: As the health care system comes under pressure to cut costs and implement more preventative care, these ideas will become more relevant. Says Dudley: “A lot of people do research on computers, but I think what we’re hoping for is that we’re going to build a health care system where complex models … are firing on an almost day-to-day basis. As patients are getting information about them put in the electronic medical record system there will be this engine in the background.”
Christian Sellars from MSD put on a terrific dinner in Crows Nest, inviting a group of interesting people to come meet with his team, with no agenda:
Dr Paul Nicolarakis, former advisor to the Health Minister
Dr Linda Swan, CEO Healthways
Ian Corless, Business Development & Program Manager, Wentwest
Dr Kevin Cheng, Project Lead Diabetes Care Project
Dr Stephen Barnett, GP & University of Wollongong
Warren Brooks, Customer Centricity Lead
Brendan Price, Pricing Manager
Wayne Sparks, I.T. Director
Greg Lyubomirsky, Director, New Commercial Initiatives
Christian Sellars, Director, Access
MSD are doing interesting things in health. In Christian’s words, they are trying to uncouple their future from pills.
After some chair swapping, I managed to sit across from Linda Swan from Healthways. It was terrific. She’s a Stephen Leeder disciple, spent time at MSD, would have been an actuary if she didn’t do medicine, and has been on a search that sounds similar to mine.
Healthways do data-driven, full-body, full-community wellness.
They’re getting $100M multi-years contracts from PHIs.
Amazingly, they’ve incorporated social determinants of health into their framework.
And even more amazingly, they’ve been given Iowa to make healthier.
They terraform communities – the whole lot.
Linda believes their most powerful intervention is a 20min evidence-based phone questionnaire administered to patients on returning home, similar to what Shane Solomon was rolling out at the HKHA. But they also supplant junk food sponsorship of sport and lobby for improvements to footpaths etc.
Just terrific. We’re catching up for coffee in January.
> 24m 30s: demonstration of a new app (closed beta) “Hospital Adviser Medicare Hip & Knee” developed by Consumer Reports (US equivalent of Choice Magazine) using publicly released de-identified cost CMS government data (if only in AU!!) – tip: don’t get your hip or knee done in NYC
> presentation by Castlight Health – US analytics business providing employees and employers personalised price & quality transparency for procedures/conditions/doctors
> The conference found that transparency is necessary but not sufficient to deliver improvements in care.
> 49m 25s: Value-based pricing – the benefit of the care, not its cost
> 50m: providers don’t have feedback on their own performance (let alone payers and patients) – when providers see their own price competitiveness, they adjust their prices
> 56m: Leapfrong asked how can transparency be applied to over-utilization of procedures? By feedback to providers.
We cannot continue on our current course without depriving other societal domains that are essential to the long-term wellbeing of our community, such as education, physical infrastructure, aged care, environmental protection, the arts and recreation
When we eventually do act we will realise that there are a limited number of ways to constrain the proportion of community resources expended on health care.
One is for funders to pay less for the things that are done.
The second, and perhaps the simplest, is to not do things that are of little or no benefit. We could also ensure that, when there is a choice, the less expensive options are used. This is primarily a task for doctors but everyone is responsible.
The third is to make sure that people do not have treatment that they do not want. This merely supports the right of people to make a choice not to start or persist with treatment that will not bring them sufficient benefit in terms of a quantity of a life of quality as they define it. This also requires community acceptance that individuals have the right to make such choices.
While thoughtful medical practice, systemic support of the right to individual choice and improved efficiency can buy us some time they are unlikely to be sufficient.
Perhaps the complex ecology of gridlocked self-interest means that struggling health systems must collapse and fail before they can be rebuilt, and we will just have to watch while it happens.
Surely a better outcome would be to work towards spending only what we can afford. These are not simple issues and the process might begin with an open discussion of our community values and the goals of health care. The sooner we start that discussion the better.